Download
1 / 1
10 likes | 366 Views
Paired Bilateral Internal Carotid Artery Aneurysms: An Imaging Review 1 Joseph R. Grajo, M.D., 2 Midhir J. Patel, B.S., 3 Raul Otero, M.D. 1 University of South Florida, Department of Radiology, Tampa, FL 2 Morsani College of Medicine, Tampa, FL 3 Radiology Associates of Tampa, Tampa, FL.

E N D
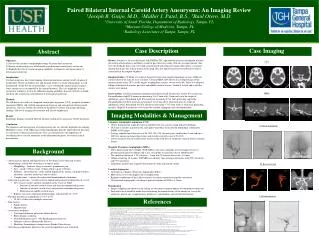
Paired Bilateral Internal Carotid Artery Aneurysms: An Imaging Review 1Joseph R. Grajo, M.D., 2Midhir J. Patel, B.S., 3Raul Otero, M.D. 1University of South Florida, Department of Radiology, Tampa, FL 2Morsani College of Medicine, Tampa, FL 3Radiology Associates of Tampa, Tampa, FL Case Imaging Abstract Case Description History: Patient is a 46 year old female with PMH of TIA, supraclinoidaneurysm and bipolar disorder presenting with headaches and blurry vision for past three days along with one syncopal episode. She rates the headache pain 6 out of 10, dull, non-localized with unknown trigger. She reports a syncopal episode but denies any falls or trauma to her head. She also reports transient vision blurriness but no central deficit or complete blindness. Imaging Studies: CT Head w/o contrast showed no acute intracranial hemorrhage or mass. MRI w/o contrast showed no signs of acute ischemia. CTA and MRA showed four focal outpouchings of the internal carotid artery (ICA) at the origins of ophthalmic arteries, two on each side. There was adequate filling of the bilateral anterior, posterior and middle cerebral arteries. Vertebral, basilar and cerebellar arteries were normal. Interventions: Cerebral angiogram confirmed and characterized the presence of four ICA aneurysms. Paraophthalmic right ICA aneurysm measuring 5.9x3.3mm with 3.3mm neck near the origin of ophthalmic artery. Paraclinoid right ICA aneurysm measuring 5.9x4.5mm projecting superiorly. Paraophthalmic left ICA aneurysm measuring 5.1x4.1mm with 4.2mm neck near the origin of ophthalmic artery. Paraclinoid left ICA aneurysm measuring 3.7x3.7mm with a 3.3mm neck projecting laterally. Right ICA aneurysms were treated by cerebral angiogram and coil embolization. Objectives 1) Discuss the incidence and pathophysiology of intracranial aneurysms. 2) Review an interesting case of bilaterally paired internal carotid artery aneurysms. 3) Highlight the role of various imaging modalities in diagnosis and management of intracranial aneurysms. Introduction Cerebral aneurysms have wide-ranging clinical presentations and are usually diagnosed incidentally. Variety in number, size and location of these vascular abnormalities is well documented. To the best of our knowledge, a case of bilaterally paired internal carotid artery aneurysms is not reported in the current literature. This case highlights such an occurrence in order to review the different imaging modalities that are currently available and their role in detection and treatment of intracranial aneurysms. MethodsWe will discuss the utility of computed tomography angiogram (CTA), magnetic resonance angiogram (MRA) and cerebral angiogram in diagnosis and management of intracranial aneurysms. Our case includes discussion of the patient’s history and unique radiologic findings. The use of imaging for treatment will also be emphasized. ResultsRadiologic findings of paired bilateral internal carotid artery aneurysms will be presented. ConclusionThe diagnosis and management of cerebral aneurysms are critically dependent on imaging. Modalities such as CTA, MRA and cerebral angiography provide unprecedented precision in evaluation of intracranial aneurysms. This case demonstrates the importance of considering these vascular anomalies in the differential diagnosis for various clinical presentations. CTA MRA Imaging Modalities & Management • Computer tomography angiogram (CTA) • CTA is performed on single-detector or multidetector row scanners using helical technology • CTA data is usually acquired in the axial plane to produce reconstructed multiplanar reformatted (MPR) or 3D images • Average reported specificity rates of 96–98% (90–94% for aneurysms smaller than 3 mm and up to 100% for aneurysms larger than 4 mm) and overall sensitivity rates of 96–98% • Lower sensitivity for the carotid artery lesions at the skull base or within the contrast-filled cavernous sinuses • Magnetic Resonance Angiography (MRA) • Three-dimensional time-of-flight (TOF) MRA is the most commonly used technique because it provides good spatial resolution and is less susceptible to signal loss due to turbulent flow • The spatial resolution of 1.5T scanner is ~1 mm and 3T scanners may reach ~0.6 mm • Volume rendering 3T scanner TOF MRA can identify 3mm or larger aneurysms with 99% sensitivity and 97% specificity • Limitations include time required to perform the study and motion artifact • Cerebral Angiogram • Also known as digital subtraction angiography (DSA) • More invasive test with higher risk of complications • Requires introduction of the catheter and use of contrast material to map the vasculature • 3D rotational angiography can enhance spatial resolution of DSA to 0.15mm • Management • Surgical clipping and endovascular coiling are two main treatment options for unruptured aneurysms • Decision to treat should be made after considering the natural history of the aneurysm, size of the aneurysm, patient age, symptomology, preference, comorbidities and risk of interventions Cerebral Angiogram Background • Aneurysms are dilated and thinned areas of the blood vessels that lead to focal outpouchings, usually due to weakness in tunica media • Morphology– fusiform, berry or saccular, pseudoaneurysm • Size – small (<10mm), large (10mm-25mm), giant (>25mm) • Etiology – atherosclerosis, cystic medial degeneration, trauma, congenital defects, infections (mycotic aneurysms) and vasculitis • Complications – rupture, dissection and thromboembolus formation • Intracranial aneurysms - saccular or berry shaped and localized at bifurcation of vessels • 85% of cases involve anterior circulation in the Circle of Willis • Junction of anterior cerebral artery and anterior communicating artery • Junction of internal carotid artery and posterior communicating artery • Bifurcation of middle cerebral artery • Rupture can cause subarachnoid hemorrhage with mortality of ~50% • Baseline prevalence in population is 0.2% to 6% • 20-30% of these have multiple aneurysms • Risk factors • Family history • Hypertension • Associated conditions • Autosomal dominant polycystic kidney disease • Ehlers Danlos syndrome • Neurofibromatosis type 1 (Von Recklinghausen Disease) • Tuberous sclerosis (Bourneville Disease) • Hereditary hemorrhagic telangiectasias (Rendu-Osler disease) • Screening asymptomatic patients in the general population is not warranted 3D Reconstruction Coil Embolization References Austin G, Fisher S, Dickson D, et al. The significance of the extracellular matrix in intracranial aneurysms. Ann Clin Lab Sci 1993; 23:97. Bederson JB, Awad IA, Wiebers DO, et al. Recommendations for the management of patients with unruptured intracranial aneurysms: A statement for healthcare professionals from the Stroke Council of the American Heart Association. Circulation 2000; 102:2300. Bederson JB, Connolly ES Jr, Batjer HH, et al. Guidelines for the management of aneurysmal subarachnoid hemorrhage: a statement for healthcare professionals from a special writing group of the Stroke Council, American Heart Association. Stroke 2009; 40:994. Hacein-Bey L, Provenzale JM. Current Imaging Assessment and Treatment of Intracranial Aneurysms. AJR January 2011 196:32-44 Huston J 3rd, Nichols DA, Luetmer PH, et al. Blinded prospective evaluation of sensitivity of MR angiography to known intracranial aneurysms: importance of aneurysm size. AJNR Am J Neuroradiol 1994; 15:1607. Li MH, Cheng YS, Li YD, et al. Large-cohort comparison between three-dimensional time-of-flight magnetic resonance and rotational digital subtraction angiographies in intracranial aneurysm detection. Stroke 2009; 40:3127. Li MH, Li YD, Tan HQ, et al. Contrast-free MRA at 3.0 T for the detection of intracranial aneurysms. Neurology 2011; 77:667. Menke J, Larsen J, Kallenberg K. Diagnosing cerebral aneurysms by computed tomographic angiography: meta-analysis. Ann Neurol 2011; 69:646. Neil-Dwyer G, Bartlett JR, Nicholls AC, et al. Collagen deficiency and ruptured cerebral aneurysms. A clinical and biochemical study. J Neurosurg 1983; 59:16. Pepin M, Schwarze U, Superti-Furga A, Byers PH. Clinical and genetic features of Ehlers-Danlos syndrome type IV, the vascular type. N Engl J Med 2000; 342:673. Rinkel GJ, Djibuti M, Algra A, van Gijn J. Prevalence and risk of rupture of intracranial aneurysms: a systematic review. Stroke 1998; 29:251. Roos EJ, Rinkel GJ, Velthuis BK, Algra A. The relation between aneurysm size and outcome in patients with subarachnoid hemorrhage. Neurology 2000; 54:2334. Schievink WI. Intracranial aneurysms. N Engl J Med 1997; 336:28. Schwartz RB, Tice HM, Hooten SM, et al. Evaluation of cerebral aneurysms with helical CT: correlation with conventional angiography and MR angiography. Radiology 1994; 192:717. Stehbens WE. Aneurysms and anatomical variation of cerebral arteries. Arch Pathol 1963; 75:45 Tidswell P, Dias PS, Sagar HJ, et al. Cognitive outcome after aneurysm rupture: relationship to aneurysm site and perioperative complications. Neurology 1995; 45:875. van Gelder JM. Computed tomographic angiography for detecting cerebral aneurysms: implications of aneurysm size distribution for the sensitivity, specificity, and likelihood ratios. Neurosurgery 2003; 53:597. White PM, Teadsale E, Wardlaw JM, Easton V. What is the most sensitive non-invasive imaging strategy for the diagnosis of intracranial aneurysms? J NeurolNeurosurg Psychiatry 2001; 71:322. Wiebers DO, Piepgras DG, Meyer FB, et al. Pathogenesis, natural history, and treatment of unruptured intracranial aneurysms. Mayo ClinProc 2004; 79:1572. Wiebers DO, Whisnant JP, Huston J 3rd, et al. Unruptured intracranial aneurysms: natural history, clinical outcome, and risks of surgical and endovascular treatment. Lancet 2003; 362:103.