Download

1 / 48
480 likes | 487 Views
Supporting Realistic Medicine through the delivery of a Single National Formulary. Welcome. Today’s session.

E N D
Supporting Realistic Medicine through the delivery of aSingle National Formulary
Today’s session In this interactive session, delegates will take part in group discussions to consider how to implement the new approach throughout Scotland by considering current practice and what will help facilitate the roll-out of the national formulary and how it can be embedded.
Realistic Medicine and the development of theScottish Formulary
Benefits of the Scottish Formulary • Support the reduction of unwarranted variation in prescribing practice, reducing medicine harm and continuing to improve patient outcomes. • Help to achieve more equitable, greater value-based care so that the potential population benefit from medicines can be maximised. • Supports the principle that services and functions of the health service which can be delivered more efficiently at national level will be done on a ‘Once for Scotland’ basis
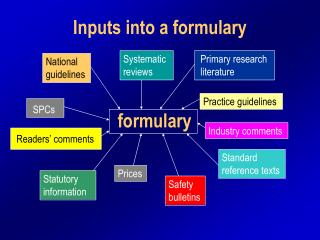
Defining the Scottish Formulary • How do the existing formularies describe themselves? “list of medicines approved for local use” “promoting high quality, safe and cost-effective prescribing” “evidence-based formulary ” “drug prescribing guidance” “provide appropriate treatment for the vast majority of patients” “based on local expert opinion and practice” “a tool to assist” “primary and secondary care”
Development approach Chapter Chapter Chapter Chapter Chapter Chapter Chapter Chapter Chapter Chapter Chapter Chapter Chapter Chapter Chapter Chapter Chapter Business As Usual Arrangements Development Process Chapter Groups Evidence & Guidance Data Analysis IT Platform Comms & Engagement SMC Decisions Appeals Process
A national approach to realising realistic medicine in antimicrobial prescribing Dr R. Andrew Seaton Consultant in Infectious Diseases, NHS GGC Chair of the Scottish Antimicrobial Prescribing Group @raseaton66
SAPG Delivering a National Antimicrobial Stewardship Programme INDIVIDUAL POPULATION OPTIMISE USE AND OUTCOME CONSORTIUM OF EXPERTS/HB AMTs ANTIMICROBIAL PRESCRIBING SURVEILLANCE QUALITY IMPROVEMENT EDUCATION
SAPG NATIONAL FORMULARY CONSENSUS GUIDELINES REDUCE VARIATION ANTIMICROBIAL PRESCRIBING OPTIMISE USE AND OUTCOME UNNECESSARY OR REDUNDANT REDUCE WASTE REDUCE HARM (AMR+) & OPTIMISE OUTCOME AMR, CDI, SAB GaV PEN ALLERGY REDUCE HARM PERSONALISE/ INDIVIDUALISE RISK-BASED DECISION SUPPORT VIA MOBILE APP.
SAPG: Reducing Harm VoL outbreak
SAPG Delivering a National Antimicrobial Stewardship Programme NATIONAL FORMULARY CONSENSUS GUIDELINES REDUCE VARIATION ANTIMICROBIAL PRESCRIBING OPTIMISE USE AND OUTCOME UNNECESSARY OR REDUNDANT REDUCE WASTE REDUCE HARM (AMR+) & OPTIMISE OUTCOME AMR, CDI, SAB GaV PEN ALLERGY REDUCE HARM PERSONALISE/ INDIVIDUALISE RISK-BASED DECISION SUPPORT VIA MOBILE APP.
Advantages of a Single National Approach – Antimicrobial Perspective • SAPG - National engagement and process for change • In line with SAPG work to date • Reducing harm, waste and unnecessary variation through consensus • “Working across borders” during training • Amplifying best practice • Avoiding duplication of effort
Challenges of a Single National Approach – Antimicrobial Perspective • Local autonomy and cross speciality consensus • Local initiatives to enhance AMS • Contingency/flexibility/response • To supply issues • To outbreaks • To new evidence • Governance of “Business as usual” • Local responsibility for guidance
% commonality BNF Chapter – NHS Board Range 96% - 97% 67% - 78% 49% - 91% Formulary is not the same as guidance (or practice) Effective Prescribing &
Primary Care • 80% of antimicrobials are prescribed within PC • PHE guidance agreed/adopted by SAPG and AMTs • De facto national consensus
Secondary Care • SAPG guidance • Principles of AMS • Surgical Prophylaxis • Gent and Vanc guidance • Variation in empirical guidance • Evolved over time • Reviewed annually/2yearly by HB AMTs
Promotion of Gentamicin-based Empirical Hospital Guidance (Sepsis)
STEWARDSHIP INITIATIVES - Learning from variation to generate change
Other considerations in national guidance in antimicrobial prescribing • Restricted/Protected status of antimicrobials: • Consensus • Duration of therapy: • Some minimal variation • IV to Oral Switch Therapy (IVOST): • Work ongoing • Approach to penicillin allergy: • National work underway
Penicillin Allergy De-labelling • 10% of inpatients “labelled” • Mislabelling in c. 80% + associated with increased Rx cost, admission length, AMR and poorer outcomes • Teicoplanin 17 xs increased risk of anaphylaxis cf other antibiotics • De-labelling complicated
Single (Scottish) National FormularyInfections Chapter • Phase 1: • Primary care (80% of antibiotic prescribing) – SAPG/AMTs • Are we there already? • HIV (HIV leads group, RakNandwani) • HCV (National group, John Dillon) • Phase 2: • Hospital prescribing – SAPG/AMTs
Conclusions • SAPG provides a national framework for AMS • Excellent engagement with board AMTs • Work programme is aligned to Realistic Medicine • Consensus in best prescribing practice in both primary and secondary care is fundamental to reducing waste, harm and unnecessary variation in practice • Good progress to date towards these goals • Needs flexibility and ability to respond to emerging challenges
Acknowledgements • SAPG SNF Group • Health Boards Busi Mooka (Tay) , Ursula Altmeyer (A&A), Anne Duguid (Borders), Bryan Marshall (D&G), Niketa Platt (Fife), Robbie Weir (FV), Sandy Mackenzie (Gramp), Brian Jones (GGC), Gail Haddock (Highland), Adam Brown (Highland), Stephanie Dundas (Lanark), Morgan Evans (Lothian), • Professional Groups: Anne Thomson (National Prescribing Adviser group), Suzanne Clark (Public Partner), Mairi MacLeod (SMVN) Jacqueline Sneddon (SAPG) and Deirdre O’Driscoll (IPCN),
13 25 9 30 29 28 27 End 1 2 3 4 5 7 8 6 24 23 22 21 20 10 18 17 19 15 14 26 12 11 16 Group discussions Time remaining: Minutes Which communication methods should be utilised when engaging with Board colleagues around implementation? (prioritise your suggestions) Which roles within your Board should we be directly communicating with regarding the implementation of the Scottish Formulary? (prioritise your suggestions) What do you feel are the key points to be considered in communications with patients around the Scottish Formulary? (prioritise your suggestions) Which existing processes within your Board should we be considering as part of the implementation plans? (consider what happens now and what processes you feel will change when the Scottish Formulary is introduced)
Thank you for your contributionKeep up to date at:http://www.therapeutics.scot.nhs.uk/SNF