Download
1 / 37
370 likes | 516 Views
7T Thalamus and MS Studies. Jason Su Sep 16, 2013. Outline. 7T Thalamus and MS studies Atrophy measures – PVF, thalamus, hippocampus Study-specific mean brain template construction with ANTS Manual -> Automatic segmentation with label fusion. 7T Studies.

E N D
7T Thalamus and MS Studies Jason Su Sep 16, 2013
Outline • 7T Thalamus and MS studies • Atrophy measures – PVF, thalamus, hippocampus • Study-specific mean brain template construction with ANTS • Manual -> Automatic segmentation with label fusion
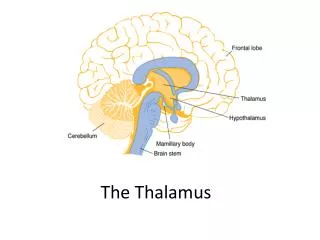
7T Studies • Thomas, Manoj, and Ives recently used WMnMPRAGE to manually segment thalamic nuclei in normal control • Now looking to use this methodology in MS patients at 7T with atrophy and disease markers: • Brain atrophy, parenchymal volume fraction • T2-FLAIR lesions • Thalamic atrophy (whole or nuclei) • Thalamic lesions • Hippocampal atrophy
Brain Atrophy • Want to measure the ratio of the brain parenchyma to the intracranial cavity volume • Previous MSmcDESPOT methodology • FSL BET the “target” image (T1w SPGR, 18deg) • The intracranial volume • Segment WM+GM MPRAGE with SPM8 • The brain parenchyma volume • Measures enlargement of ventricles mainly
T1w BET T1w-MPRAGE T2-CUBE
Brain Atrophy: New Method • FSL BET T2-CUBE image • Then edit to produce intracranial volume (~30min) • Remove CSF by segmenting T2-CUBE w/ SPM8 • Note that T1w input is more typical for SPM8 but CSF is so distinct on T2w it works • Then edit to produce brain parenchyma • Advantages: • More true to the definition of intracranial cavity • Better measure of the space between brain and skull
T2w BET After Editing Before Editing
CSF Removal After Editing Before Editing ?
Difficulties • SPM8 is the weakest part of the pipeline • Often needs manual tweaking between subjects to get to a reasonable segmentation • Registration to its atlas often goes haywire, likely affected by 7T nonuniformity • Would be easy to manually threshold bright voxels as CSF but reviewers might prefer a proven toolbox • Is it better to be consistent or accurate? • Does it matter in the end since always edited as a final step?
T2-FLAIR Lesions • Previous MSmcDESPOT methodology • Nonlinearly register all subjects to MNI brain • Normalize signal intensities to “robust” max in brain • Group normal controls and find their voxel-wise mean and std. dev. • Compare new subject to the control population • Voxels > 4 standard deviations above mean = lesion • Voxels > 2 standard deviations above mean = DAWM
T2-FLAIR Lesions • New methodology • Create a study-specific mean brain template to use instead of MNI • More accurate registration should improve ability to detect lesions, maybe cortical?
Mean Brain Template • ANTs (Advanced Normalization Tools) is emerging as the standard • Available in pre-compiled OSX binary • Provides useful parallelized script to compute a mean brain (buildtemplateparallel.sh) • But sometimes crashes whole computer! • Which image contrast? Want something that: • Provides useful image contrast throughout the brain • Is less affected by B1+ inhomogeneity, as this variation between subjects is not taken into account in these registration algorithms • Do typically correct for receive nonuniformity • Shows few lesions so they do not misguide the registration
MPRAGE • Good gray/white contrast throughout brain • Uniformity isn’t ideal • Shows few lesions
WMnMPRAGE • Extreme gray/white contrast throughout brain • Uniformity seems better than MPRAGE, could be visual effect due to extreme contrast • Shows some lesions
T2-CUBE • Poor gray/white contrast • Decent uniformity • Shows few lesions
FLAIR • Decent contrast • Uniformity is poor, signal loss in center of brain, which we care about the most for thalamus • Shows many lesions
Decision • My first attempt was with WMnMPRAGE • Good contrast albeit unusual, but registration algorithms should be indifferent to that • Most importantly, this is the contrast we’re using for thalamic segmentation so it is a natural choice
ANTs • Sum all subject brains without registration creating a crude template • Rigidly register subjects to this crude base • Sum these to produce the initial template • Iterate until convergence: • Nonlinearly register to the template • Sum the new registrations to create a new template
ANTs Iteration 1
ANTs Iteration 2
ANTs Iteration 3
ANTs Iteration 7
ANTs Iteration 8
Notes • Cortical registration seems good • Still not quite converged after 8 iterations • 4 is the default number of iterations, way low • Each iteration takes 12 hours, barring any crashes • Once this is settled, can do segmentation of the lesions • Comparing FLAIR intensities to controls is fairly straightforward • May want to also do it on WMnMPRAGE for thalamic lesions
Structural Atrophy • After our review of label fusion and ASHS papers, learned we can turn previous manual segmentations into automatic • Thomas has already manually segmented 2x6 controls, though in a non-accelerated WMnMPRAGE • Label fusion: • Register the previous segmentations to the new subject • Use local information about the registration accuracies to guide the decision
What We Want Prior Subject 1 Prior Subject 2 Prior Subject 3 New Subject
Problem • Nonlinear registration of N prior subjects is expensive to every new subject • Instead use the mean brain template as an intermediate space • Allows us to only need one registration for a new subject
Proposed Approach Prior Subject 1 Prior Subject 2 Prior Subject 3 Mean Brain Template New Subject
Drawbacks • Not straightforward how to adapt this to an ROI-focused registration • Accuracy of the mean template may be imperfect due to the expense of registering whole brain • As in ASHS, would like to first start from the whole brain registration • Then do a targeted registration with small FOV on thalamus or hippocampus • Do we take brains all the way to the subject space and register there or stay in the template space? • ASHS chooses to use template space, less intuitive • Argument for it has to do with producing a label probability map which plays nicely with linear interpolation unlike a binary mask • But STEPS does not expose that intermediate map
Other Concerns • STEPS suggested a library in the range of 15+ subjects • May not be able to achieve reliable automatic segmentation until after the study • Before that we can at least try to get something reasonable to reduce Thomas’s tracing work
Nuclei Separability by T1 • Another possibility is to incorporate T1 map information to help improve label fusion • Possibly as an included variable in AdaBoost like ASHS
Notes • For 3/5 nuclei, the T1 dist. is distinct from some or all of its neighbors