Download
1 / 19
210 likes | 572 Views
Thyroid Nodules. Hollis Moye Ray, MD SEAHEC Internal Medicine June 3, 2011. Thyroid Nodules. Palpable: 4 – 7% Detected on ultrasound: 20 – 65% More common: aging, women Cancer risk: 5 – 10%. Benign Causes. Multinodular (sporadic) goiter ("colloid adenoma")

E N D
Thyroid Nodules Hollis Moye Ray, MD SEAHEC Internal Medicine June 3, 2011
Thyroid Nodules • Palpable: 4 – 7% • Detected on ultrasound: 20 – 65% • More common: aging, women • Cancer risk: 5 – 10%
Benign Causes • Multinodular (sporadic) goiter ("colloid adenoma") • Hashimoto's (chronic lymphocytic) thyroiditis • Cysts: colloid, simple, or hemorrhagic • Follicular adenomas • Macrofollicular adenomas • Microfollicular or cellular adenomas • Hurthle-cell (oxyphil-cell) adenomas • Macro- or microfollicular patterns
Malignant Causes • Papillary carcinoma • Follicular carcinoma • Minimally or widely invasive • Oxyphilic (Hurthle-cell) type • Medullary carcinoma • Anaplastic carcinoma • Primary thyroid lymphoma • Metastatic carcinoma (Breast, renal cell, others)
Thyroid Cancer • Lower prevalence in • “Hot nodules” • Multinodular goiters • Higher prevalence in • Male • Children • Adults < 20 or > 60 years old • History of head/neck irradiation • Family history of thyroid cancer • Rapid growth • Hoarseness
Evaluation • History • Rapid growth? • Family history? • Irradiation? • Cancer syndromes? • Physical Examination • Fixed, hard mass • Vocal cord paralysis • Cervical lymphadenopathy • Obstructive symptoms
Evaluation • TSH • Low Thyroid scintigraphy • Not low US to select for FNA biopsy; evaluate for hypothyroidism • Ultrasound • High risk of cancer: hypoechoic, microcalcifications, increased central vascularity, irregular margins, taller than wide, documented enlargement, size >3cm • Low risk of cancer: hyperechoic, peripheral vascularity, pure cyst, comet-tail shadowing
Evaluation • Thyroid Scintigraphy • Select nodules for FNA • Uses radioisotope to detect “hot” and “cold” • Most benign and virtually all malignant thyroid nodules are “cold” (take up less/no isotope) • Helps to guide FNA biopsy
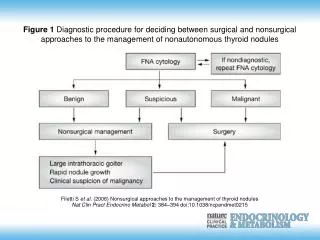
Evaluation • FNA biopsy • Procedure of choice • Safe and simple • 90 – 95% of sensitive • False negative rate only 1 – 11% • What to biopsy? Basically all >1cm EXCEPT • Spongiform nodules < 2cm • Purely cystic nodules
Other Lab Tests • Calcitonin • Controversial – consider if hypercalcemic, family history, or MEN type 2s • Anti-TPO Antibodies • Only recommended if suspicious for autoimmune disease (i.e. Hashimoto’s) • Thyroglobulin • Does not discriminate benign from malignant • Can be useful s/p thyroidectomy or ablation
Diagnostic Categories • Benign —macrofollicular or adenomatoid/hyperplastic nodules, colloid adenomas, nodular goiter, and Hashimoto's thyroiditis. • Follicular lesion of undetermined significance — lesions with atypical cells, or mixed macro- and microfollicular nodules. • Follicular neoplasm —microfollicular nodules (i.e. Hurthle cell lesions) • Suspicious for malignancy • Malignant • Nondiagnostic
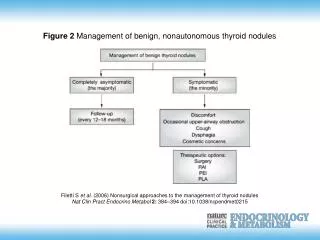
Benign Nodules • Macrofollicular or adenomatoid/hyperplastic nodules, colloid adenomas, nodular goiter, and Hashimoto's thyroiditis • Followed without surgery • T4 therapy (?) – MAY decrease size, prevent further growth • Periodic ultrasound monitoring • Repeat aspiration if change in size, texture, or new symptoms
Follicular lesion of undetermined significance • Nodules with atypical cells, nodules w/ both macro and microfollicular features • Risk of malignancy: 5-10% • Excision: no definite consensus • ? Follow with aspiration - if atypical cells found, then excise
Follicular neoplasm (microfollicular) • If TSH normal – typically surgery • If TSH low - perform thyroid scintigraphy • If hyperthyroid – radioiodine tx or surgery • Hyperfunctioning (autonomous) – followed • Non-autonomous – surgery w/path eval for vascular or capsular invasion • 15 – 25% cancerous
Malignancy = Surgery* • Papillary and Follicular - well-differentiated and good prognosis if in early stage • Medullary • Anaplastic – poorly differentiated and aggressive • Metastatic • Suspicious for malignancy – surgery • 50 – 75% malignant • *Thyroid lymphoma – the exception • Radiation, not surgery!
Management of other path findings • Nondiagnostic FNA – repeat under US • Cystic thyroid nodules – followed or excised for therapeutic reasons if recurrent • Ablation – benign, autonomous, or cystic • Inject ethanol or other sclerosing agent • Controversial (complications, prolonged pain)
References • MKSAP 15: Endocrinology and Metabolism • Harrison’s Internal Medicine • UpToDate: Thyroid Nodules