EMG II
470 likes | 1.11k Views
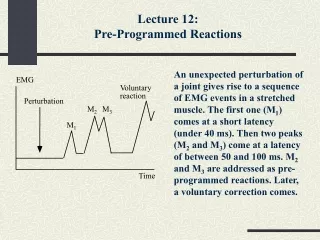
EMG II. Academic half-day 2008 Dr. Fraser Moore fraser.moore@mcgill.ca. QUESTIONS FROM LAST TIME ?. Axon loss Demyelination Conduction block Amplitude Latency Conduction velocity. Neuropathy Localization Motor/sensory Axonal Demyelinating . NCS BOTTOM-LINE. TODAY Needle EMG.

EMG II
E N D
Presentation Transcript
EMG II Academic half-day 2008 Dr. Fraser Moore fraser.moore@mcgill.ca
Axon loss Demyelination Conduction block Amplitude Latency Conduction velocity Neuropathy Localization Motor/sensory Axonal Demyelinating NCS BOTTOM-LINE
TODAY Needle EMG NEXT TIME V. Late responses VI. Neuromuscular Junction PLAN
IV. NEEDLE EMG Insertional activity Activity at rest Motor unit potentials Disorders Limitations Report
WHY DO WE DO THE NEEDLE EXAM ? • Help to localize • Identify chronicity and prognosis • Distinguish between neuropathy and myopathy
NEEDLE EXAM • Observe electrical activity of muscle: • With needle mvmt • At rest • With vol. activation • Motor unit potentials
1. INSERTIONAL ACTIVITY • Discharges of muscle fibers irritated by passage of needle • Increased with increased irritability of muscle fibers
2. ACTIVITY AT REST • Fibrillations and positive sharp waves • Spontaneous firing of individual muscle fibers (muscle fiber action potentials)
3. MOTOR UNIT POTENTIALS • Summation of all muscle fiber action potentials of one motor unit • Amplitude depends on nearby fibers • Duration depends on all fibers • Phases depend on timing therefore…* Will change with change in needle position. (Note: MUP = MUAP)
MOTOR UNIT POTENTIALS • Amplitude • Duration • Phases • Stability • Recruitment
4. DISORDERS Axonal injury: a dynamic process ! • Loss MUAP’s = decreased recruitment • Denervation = fibrillations
4. DISORDERS Axonal injury: a dynamic process ! • Loss MUAP’s = decreased recruitment • Denervation = fibrillations • Initial reinnervation = long, polyphasic • Maturation = large
MOTOR UNIT POTENTIALS • Amplitude • Duration • Phases • Stability • Recruitment
4. DISORDERS cont… Myopathy = loss of muscle fibers, so MUAPs are: • Smaller amplitude, shorter duration • Polyphasic • Fast recruitment but…* Inflammation = fibrillation Hypertrophy = Larger amplitude
MOTOR UNIT POTENTIALS • Amplitude • Duration • Phases • Stability • Recruitment
COMPARISON Neuropathy Myopathy Fibrillations present absent MUP Amplitude increased decreased MUP Duration long short Polyphasic yes yes “neurogenic” “myogenic” But… “dynamic” exceptions Recruitment decreased increased
5. LIMITATIONS • Choice of muscles • Time spent on each muscle • Needle position A subjective test !
6. NEEDLE EXAM REPORT* Insertional Fibrillations Ampl. Dur. Recruitment Notes Muscle 1 + N poly Muscle 2 ++ N v. poly Muscle 3 N 0 N N N Muscle 4 N 0 N N N Muscle 5 N 0 N N N (Note: the report will usually concentrate on abnormal motor units. For example, muscles 1 and 2 could also have many normal motor units)
MFAP MUAP CMAP Localize Chronicity/Prognosis Neuropathy vs. Myopathy NEEDLE EXAM BOTTOM LINE
CASES (Part I and Part II)
1. CARPAL TUNNEL SYNDROME • Technique: -median and ulnar conductions -motor and sensory • Pathophysiology: -compression -demyelination -axon loss From JAMA 2000;283:3110
THREE QUESTIONS • Does the needle exam help ? • How can we get more “precise” and sensitive? • Any other ways?
2. ULNAR NEUROPATHY AT THE ELBOW • Pathophysiology: -compression, demyelination, axon loss • Look for focal slowing across elbow • If axonal, may not be able to localize*
ELBOW WRIST
LIMITATIONS OF NEEDLE EXAM • May be demyelinating • Can see fascicular involvement • No ulnar muscles above elbow • 2 sites of ulnar involvement at the elbow*
3. MYOPATHY • Normal or diminished CMAP • Fibrillations if inflammatory • Small, short, polyphasic MUAPs • Large MUAP’s if hypertrophy • Increased recruitment
MYOPATHY cont… “Rule out myopathy” doesn’t work well: -patchy involvement of muscle fibers, we look at motor units -can see increased amplitude, can see fibs -recruitment difficult to judge
UNUSUAL FINDINGS • Complex repetitive discharge • Sudden start and stop, fixed morphology, MFAPs • Myotonic discharge • Wax and wane, MFAPs • Myokymic discharge • Rhythmic firing of single MUAP • Neuromyotonic discharge • Non-rhythmic, extremely rapid firing of single MUAP
Axon loss Demyelination Conduction block Amplitude Latency Conduction velocity Neuropathy Localization Motor/sensory Axonal Demyelinating NCS BOTTOM-LINE
MFAP MUAP CMAP Localize Chronicity/Prognosis Neuropathy vs. Myopathy NEEDLE EXAM BOTTOM LINE
REMEMBER… History, NE, NCS, needle exam interpreted together (if something doesn’t fit, start over)
TAKE HOME MESSAGE • Ask a specific question when you order an EMG • Interpret the report • Was the appropriate testing done? • Are the conclusions appropriate for the results ? • Think beyond positive or negative • Think anatomy and pathophysiology
REFERENCES • Aids to the examination of the peripheral nervous system. • ISBN 0-7020-2512-7 • Good overview
REFERENCES • Stewart J. • Focal Peripheral Neuropathies • ISBN 0-7817-1717-5 • Much better for nerves
REFERENCES • Katirji B. • Electromyography in clinical practice. A case study approach. • ISBN 0-8151-4971-9
REFERENCES • Preston and Shapiro. • Electromyography and Neuromuscular Disorders. Clinical-electrophysiological correlations. • ISBN 0-7506-7492-X
REFERENCES AAEM Minimonographs (Muscle+Nerve) Glossary of terms (Oct 1987) Waveforms (Oct 1987) Motor unit recruitment (1991;14:489) Nerve Injury (2000;23:863) Radiculopathy (1988;11:1099) (and others…)
REFERENCES Chalk CH. Acquired peripheral neuropathy. Neurol Clinics 1997; 15: 501. Practice parameter for electrodiagnostic studies in carpal tunnel syndrome. Muscle and Nerve 2002;25:918. Stewart JD. The variable clinical manifestations of ulnar neuropathies at the elbow. JNNP1987; 50: 252. Campbell WW. Evaluation and management of peripheral nerve injury. Clin Neurophysiol 2008; 119: 1951.
REFERENCES Dumitru Electrodiagnostic medicine ISBN 978-1560534334 Kimura Electrodiagnosis in diseases of nerve and muscle ISBN 978-0195129779 Use these as references if you have specific (technical) questions