Download
1 / 42
420 likes | 528 Views
You are here. The Big Picture: An Overview of Major Events Shaping National, State, Public and Private Cessation Policy Matt Barry Director, Policy Research Campaign for Tobacco Free Kids Washington, DC. What’s on the Radar? What SHOULD We Be Doing? Medicare Medicaid

E N D
You are here. The Big Picture: An Overview of Major Events Shaping National, State, Public and Private Cessation Policy Matt Barry Director, Policy Research Campaign for Tobacco Free Kids Washington, DC
What’s on the Radar? • What SHOULD We Be Doing? • Medicare • Medicaid • Other Federal Programs • State Insurance Mandates • DOJ • Varenicline and Rimonabant • Other • X Factors
What SHOULD We Be Doing? According to CDC’s Task Force on Community Preventive Services, interventions should include restrictions on exposure to secondhand smoke, increases in the unit cost of tobacco, mass media campaigns, provider reminder systems, reducing out-of-pocket expenses, and telephone counseling/support. Source – AJPM, 2001;20(2S), “Recommendations Regarding Interventions to Reduce Tobacco Use and Exposure to Environmental Tobacco Smoke”, http://www.thecommunityguide.org/tobacco/tobac-AJPM-recs.pdf.
What SHOULD We Be Doing? • Strategies to Reduce Exposure to Secondhand Smoke • Smoking bans and restrictions: strongly recommended. “Strong scientific evidence that they reduce exposure to ETS (1) in a wide range of workplace settings and adult populations; (2) when applied at different levels of scale, from individual businesses to entire communities; and (3) whether used alone or as part of a multi-component community or workplace intervention.” • Strategies to Reduce Tobacco Use Initiation • Increasing the unit price for tobacco products: strongly recommended. “Strong evidence of effectiveness in reducing tobacco use prevalence in study populations of adolescents and young adults … In addition, increasing the price for tobacco products is also effective in (1) reducing population consumption of tobacco products, and (2) increasing tobacco use cessation.” • Mass media campaigns: strongly recommended (when combined with other interventions). “Strong evidence of effectiveness in reducing tobacco use prevalence among adolescents when implemented in combination with tobacco price increases, school-based education, and/or other community education programs.”
What SHOULD We Be Doing? • Strategies to Increase Tobacco Use Cessation • Increasing the unit price for tobacco products: strongly recommended. “Strong evidence of effectiveness in (1) reducing population consumption of tobacco products, (2) reducing tobacco use initiation …and (3) increasing tobacco cessation. Excise tax increases demonstrated evidence of effectiveness in a variety of populations and when implemented at both the national and state levels.” • Mass Media Education • Campaigns: strongly recommended (when combined with other interventions). “Strong evidence of effectiveness in (1) reducing population consumption of tobacco products, and (2) increasing cessation among tobacco product users.”
What SHOULD We Be Doing? • Health Care System-Level Interventions • Provider reminders: recommended. “Provider reminders are recommended (1) whether used alone or as part of a multi-component intervention … (2) across a range of intervention characteristics (chart stickers, checklists, and flowcharts), and (3) in a variety of clinical settings and populations.” • Provider reminder plus provider education, with or without patient education: strongly recommended. “Strongly recommended on the basis of strong evidence that this combination (1) increases provider delivery of advice to quit to tobacco using patients, and (2) increases patient tobacco use cessation.” • Reducing patient out-of-pocket costs for effective cessation therapies: recommended. “Recommended … on the basis of sufficient scientific evidence of effectiveness in (1) increasing use of the effective therapy, and (2) increasing the total number of tobacco-using patients who quit.” • Multicomponent patient telephone support: strongly recommended. “Strongly recommended …on a strong body of evidence that this combination intervention (1) increases patient tobacco cessation, and (2) is effective in both clinical settings and when implemented community-wide.”
Nice Theory, But Does It Work? • Ask New York City • What did they do? • Comprehensive Smoke Free Law • Highest Cigarette Excise Tax In the U.S. • Well-Funded State Tobacco Control, Prevention and Cessation Program (including quitline and quit clinics) • The results? • In one-year, an 11% drop in adult smoking rates between 2002-2003 (from 22% to 19%). • 100,000 fewer smokers.
Medicare • March 22, 2005 - CMS issued a final decision memo to cover tobacco cessation counseling services under Part B. • Counseling services are now available to all beneficiaries with a disease or an adverse health effect linked to tobacco use or who are taking a therapeutic agent that is affected by tobacco use. • Medicare now covers 2 cessation attempts per year - a maximum of 4 intermediate or intensive sessions, with the total annual benefit up to 8 sessions. Source: Decision Memo for Smoking & Tobacco Use Cessation Counseling (CAG-00241N), March 22, 2005,http://www.cms.hhs.gov/mcd/viewdecisionmemo.asp?id=130.
Medicare – Next Steps • Need to promote awareness of this benefit among beneficiaries and providers. • Need to promote awareness of this decision by CMS among other public and private insurers. • Need to work with CMS and/or Congress to allow access by beneficiaries to telephone quitline services – quitlines are not eligible for reimbursement under the CMS decision. • Need to coordinate this benefit with prescription drug benefit taking effect January 2006. • Need to work with CMS on training/certification of providers. Source: Decision Memo for Smoking & Tobacco Use Cessation Counseling (CAG-00241N), March 22, 2005,http://www.cms.hhs.gov/mcd/viewdecisionmemo.asp?id=130.
Other Federal Activity Federal Employees Health Benefit Plan - In an August 7, 2003 memo to Rep. Meehan, former OPM Director Kay Cole James stated: “I continue to encourage FEHBP plans to provide benefits for programs aimed at health promotion and disease prevention, including smoking cessation programs … While we urge plans to cover special benefits and programs, we do not mandate that they do so …” [For more information on FEHBP, see http://www.opm.gov/insure/health/index.asp] Federal Bureau of Prisons – Effective July 15, 2004 – “1. [PURPOSE AND SCOPE §551.160. To advance towards becoming a clean air environment and to protect the health and safety of staff and inmates, the Bureau of Prisons will restrict areas and circumstances where smoking is permitted within its institutions and offices.]” [For more information on BOP no smoking policy, see - http://www.bop.gov/] Department of Veterans Affairs – The VA published an interim final rule in the Federal Register on May 2, 2005, to “… amend its medical regulations concerning co-payments for inpatient hospital care and outpatient medical care. This rule designates smoking cessation counseling (individual and group sessions) as a service that is not subject to co-payment requirements. The intended effect of this interim final rule is to increase participation in smoking cessation counseling by removing the co-payment barrier.” [For more information on VA cessation programs and policies, see - http://www.publichealth.va.gov/smoking/describe.htm and http://www.va.gov/smokingmh/index.html]
Current CMS Federal/National Policy On Cessation for Medicaid • General Policy - • Smoking cessation benefits, such as counseling and drug therapy, are optional benefits under Medicaid (except for kids covered under EPSDT). • Smoking cessation drugs are specifically classified as those drugs that may be excluded from coverage under Medicaid. • Smoking cessation counseling services may be provided under a variety of Medicaid benefit categories. • Pregnant Women - There are no mandatory smoking cessation benefits for pregnant women under Medicaid. A state may elect to provide smoking cessation services in a State plan.
Medicaid – State Activity It’s ugly out there folks …
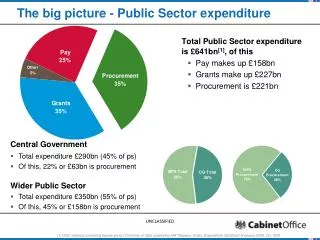
Despite the crushing financial burden of Medicaid on State budgets … “… Medicaid growth continues to outpace every other functional category of state expenditure, increasing by 8 percent in fiscal 2003; Medicaid now totals 21.4 percent of all state spending.” “Total Medicaid spending in fiscal 2003 excluding administrative costs was $243.6 billion ...” Source: National Association of State Budget Officers, 2003 State Expenditure Report, http://www.nasbo.org/Publications/PDFs/2003ExpendReport.pdf.
… there is hope!!!!! • For Example • The State of Kentucky had a projected $200 million budget deficit for FY 2005(Source: Center for Budget and Policy Priorities, State Budget Deficits Projected For FY 2005, http://www.cbpp.org/10-22-03sfp2.htm). • Despite this deficit, a NEW tobacco cessation benefit for pregnant women was added to the Medicaid program. • Our message? It saves lives, it saves money and it works. • How did this happen? Good luck, great facts, and great work by the state coalition, state officials and legislators. • If it can happen in Kentucky, it can happen anywhere.
Tobacco Dependence Treatment 2002 2003 Zyban 40 36 Nasal Spray & Inhaler 28 27 Patch 27 28 Gum 26 27 Individual Counseling 17 14 Group Counseling 10 11 Telephone Counseling 5 4 Number of State Medicaid Programs Covering Tobacco Dependence Treatments (N=51), 2003 Source: Halpin, HA, MMWR, January 30, 2004 / 53(03);54-57. Source: Analysis by the Center for Health and Public Policy Studies, University of California at Berkeley of the State Medicaid Tobacco Dependence Treatment Survey, 2003. http://statehealthfacts.org/cgi-bin/healthfacts.cgi?action=compare&category=Health+Status&subcategory=Smoking&topic=Cessation+Treatment+Under+Medicaid.
Informing Medicaid Tobacco Users about Benefits, 2003 Source: Analysis by the Center for Health and Public Policy Studies, University of California at Berkeley of the State Medicaid Tobacco Dependence Treatment Survey, 2003. http://statehealthfacts.org/cgi-bin/healthfacts.cgi?action=compare&category=Health+Status&subcategory=Smoking&topic=Cessation+Treatment+Under+Medicaid.
COVERAGE CONSISTENT WITH PHS GUIDELINES • 9 States Offer Comprehensive* Coverage: • California • Indiana • Maine • Minnesota • New Jersey • New York • Oregon • Pennsylvania • West Virginia * = Zyban, NRT Gum, Patch, Nasal Spray, Inhaler, and at least one type of counseling (individual, group or proactive telephone). Source: Halpin, HA, MMWR, January 30, 2004 / 53(03);54-57.
State Insurance Mandates • New Mexico – Is the first state to mandate comprehensive tobacco cessationbenefits by all health care insurers (except Medicaid) – effective 3/1/04. The benefit includes: • Diagnostic services: Diagnostic services necessary to identify tobacco use, use-related conditions and dependence. • Pharmacotherapy: Two 90-day courses of prescription-only medications per calendar year. • Cessation counseling: A choice of cessation counseling of up to 90 minutes total provider contact time or two multi-session group programs per calendar year. • California – A bill (SB 576) was passed in the California legislature (Senate and Assembly), but vetoed by the Governor, that would have required health plans and insurers to cover the following tobacco cessation services: • Counseling (4 sessions of at least 30 minutes each), • All Rx and OTC cessation medications, • Two quit attempts per year. • Maryland – New mandate (HB 303 signed by the Governor 5/10/05) requiring certain insurers to provide coverage for prescription-only cessation drugs (eff. 10/1/05).
Trial phase concluded in early June 2005. • In light of major and unexplained changes to DOJ’s own cessation remedy, several public health groups (TFK, ACS, ALA, ANR, AHA, NAATPN) sought to intervene in the case. • The Court granted the motion to intervene in July 2005. Interveners have since filed their own proposed remedies with the Court (8/31/05) and a reply brief (9/26/05). • The case brings with it an opportunity and the potential for significant funding for cessation services for all smokers in the U.S. Conversely, there exists substantial risk for a bad settlement. • There remain several issues under appeal that could have a major impact on the potential financial and non-financial remedies available. • If no settlement takes place, a ruling on liability is expected by late 2005, early 2006. There Are Risks & Opportunities …
NEW DRUGS!! Varenicline and Rimonabant
Varenicline (Pfizer) and Rimonabant (Sanofi-Adventis) are two new drugs that FDA is expected to approve in the next 6 to 18 months. • Both are in late stage clinical trials and publicly available data thus far suggests that quit rates are at least as high as currently available NRTs. • The buzz around these drugs is “block buster” that could result in extensive, high profile media. • Regardless of your views on pharmacotherapy/NRT, this will provide a unique opportunity to discuss cessation issues with a variety of audiences and we must be prepared to take advantage of this opportunity when it happens.
Other Activities National Quitline Network: 1-800-QUITNOW Tax and Smokefree Activity Increased Private Sector Interest in Tobacco “X” Factors
National Quitline Network: • 1-800-QUITNOW • Has been in effect since November 2004 (approx. 156,000 callers through October 2005). • Very little $$ for promotion or actual services. • Has the potential to serve as the portal for a much more ambitious and comprehensive quitline network. • Funding at the federal level has been nominal and, as a result, the potential impact limited.
Tax and Smokefree Activity • ... they keep going, and going, and going ... • 57 state tax increases since January 2002 (12 in 2005) • 25% of U.S. population covered by comprehensive smokefree laws. • Sources: Campaign for Tobacco Free Kids, Cigarette Tax Increases By State State Per Year 2000-2005, http://www.tobaccofreekids.org/research/factsheets/pdf/0275.pdf; Americans for Nonsmokers Rights Foundation, Summary of United States Population Protected by 100% Smokefree Laws, http://www.no-smoke.org/pdf/percentstatepops.pdf.
Recent Cigarette Tax Increases WASHINGTON 202.5 MONTANA 170 MAINE 200 NORTH DAKOTA 44 VT:119 MINNESOTA 123 OREGON 118 VT IDAHO 57 NH: 80 WISCONSIN 77 SOUTH DAKOTA 53 NEW YORK 150 MA MA:151 WYOMING 60 RI:246 MICHIGAN 200 CT CT:151 IOWA 36 PENNSYLVANIA 135 NJ:240 NEBRASKA 64 NEVADA 80 OHIO 125 DELAWARE:55 UTAH 69.5 IN 55.5 ILLINOIS 98 WV 55 30 VIRGINIA MARYLAND:100 COLORADO 84 KANSAS 79 MISSOURI 17 DC:100 87 KENTUCKY 30 CALIFORNIA NORTH CAROLINA 30 TENNESSEE 20 OKLAHOMA 103 ARKANSAS 59 ARIZONA 118 NEW MEXICO 91 SOUTH CAROLINA 7 GEORGIA 37 ALABAMA 42.5 MS 18 TEXAS 41 36 LOUISIANA ALASKA 160 FLORIDA 33.9 HAWAII 140 States that have recently passed or implemented a cigarette tax increase (since 1/1/2002) Oregon actually decreased its cigarette tax by 10 cents on 1/1/04. The second phase of the North Carolina tax increase (an additional 5-cents) will be effective 7/1/06, bringing the NC tax to 35 cents per pack. November 1, 2005
Smoke-Free Laws Restaurants and Bars Restaurants June 2005
Increased Private Sector Interest in Tobacco • There is an increasing recognition of the negative financial impact of tobacco on the corporate bottom line. • Companies are tired of wasting scarce resources on spiraling health care costs and desperately want to do something about it.
Increased Private Sector Interest in Tobacco • There is a slow but growing realization of the positive impact of tobacco control policy changes (e.g., tax increases, smokefree laws) on corporate financial performance. • Tobacco control can be part of the solution to their problem. • “By Jove, I think she’s got it!”
Increased Private Sector Interest in Tobacco Is this good or bad? “… the fact is, federal and state laws prohibit employers from discriminating on the basis of age, sex, race, weight, national origin and other attributes -- and smoking is not a civil right. It's just a poor personal choice.” - Howard Weyers, CEO, Weyco, Inc.
Peter Jennings • The recent death of ABC Nightly News Anchor Peter Jennings has generated a significant amount of coverage in the media about smoking, lung cancer and the importance of quitting. • This is a “teachable moment” for many people and organizations – consumers, the media, policy makers, health care professionals, health plans/insurers/organizations. • We always need to be prepared for, and “take advantage” of, in a positive and respectful manner, the good that can come out of one individual’s personal tragedy.
In response to the death of Peter Jennings, ABC News launched a month-long series (November 2005) of stories on ABC World News Tonight and on Good Morning America about the harms associated with tobacco use, about how to quit using tobacco, and about lung cancer. • The resources include on-air stories, a dedicated website, partnerships with major public health organizations, and publicizing of cessation resources, including the national quitline number 1-800-QUIT NOW. • This is unprecedented.
Hurricane Katrina • In a recent webcast to investors, U.S. Smokeless Tobacco Company cited Hurricane Katrina and its impact on higher gasoline prices for a substantial, negative impact on sales, particularly in the Gulf Coast region. • According to UST, nearly 2/3 of its sales occur at retail convenience stores and nearly 4 out of every 5 of those stores sell gasoline. UST’s customers are trying to save money on gasoline (like the rest of us) and are making fewer stops at these stores thereby resulting in fewer sales. • Conversely, in the wake of 9/11 we saw an increase in the number of tobacco users (as well as alcohol and other substances of abuse).
Domestic Cigarette Advertising and Promotional Expenditures 1998 - 2003(Billions of dollars) $15.15 Billion $12.47 Billion $11.22 Billion $9.59 Billion $8.24 Billion $6.73 Billion Source: Federal Trade Commission Cigarette Report for 2003
Contact Information Matt Barry Campaign for Tobacco Free Kids 1400 I Street, NW – Suite 1200 Washington, DC 20005 (202) 296-5469 (202) 296-5427 (fax) mbarry@tobaccofreekids.org www.tobaccofreekids.org