Download
1 / 23
230 likes | 397 Views
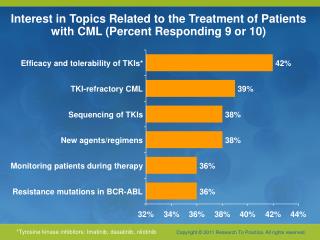
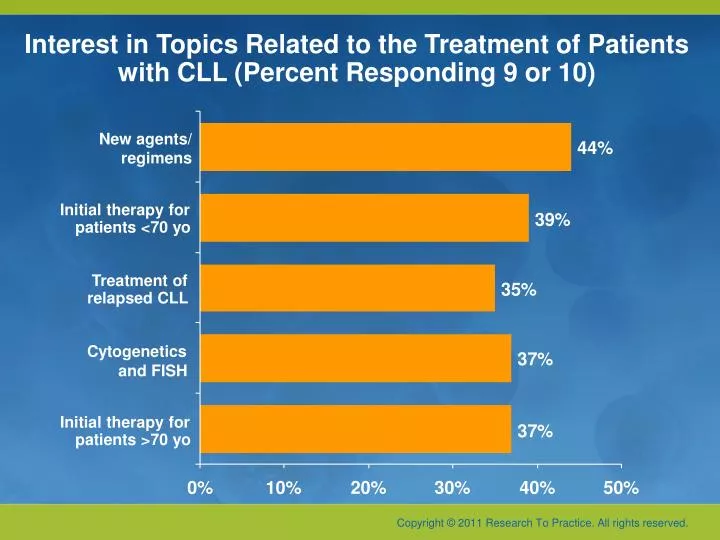
Interest in Topics Related to the Treatment of Patients with CLL (Percent Responding 9 or 10). New agents/ regimens. 44%. Initial therapy for. 39%. patients <70 yo. Treatment of. 35%. relapsed CLL. Cytogenetics. 37%. and FISH. Initial therapy for. 37%. patients >70 yo. 0%. 10%.

E N D
Interest in Topics Related to the Treatment of Patients with CLL (Percent Responding 9 or 10) New agents/regimens 44% Initial therapy for 39% patients <70 yo Treatment of 35% relapsed CLL Cytogenetics 37% and FISH Initial therapy for 37% patients >70 yo 0% 10% 20% 30% 40% 50%
State of the Art Management of Chronic Lymphocytic Leukemia Michael Hallek University of Cologne
Professional Experience Required to “Tailor” CLL Therapy: Characteristics at Presentation • Median age at diagnosis: 72 years1 • Elderly patients may be fit or have comorbidities Mean no. of co-morbidities n/a 2.9 4.2 3.6 1Ries LAG et al. SEER Cancer Statistics Review 1975–2005.2 Yancik R. Cancer 1997; 80:1273–83.
Classification of Patients by a Comprehensive Geriatric Assessment (CGA) Suitable for standard treatment GO Cumulative Illness Rating Scale Suitable for reducedtreatment SLOW Suitable for supportive care NO Gribben JG. Blood 2009;114:3359-60; Balducci L, Extermann M. Oncologist 2000;5:224-37.
Comparison of Fludarabine (F), Bendamustine (Ben), Alemtuzumab (Al) and Chlorambucil (Chl) as Single Agents 1 Rai KR et al. N Engl J Med 2000;343:1750–57. 2 Hillmen P et al. J Clin Oncol 2007;25:5616–23.3 Knauf W et al. J Clin Oncol 2009;27:4378-84.
CLL5 Protocol, Patients >65 Years (Median 70)Eichhorstet al, Blood 114, 3382 (Oct 15, 2009) 193 patients were randomly assigned to receive fludarabine 25 mg/m2 (5d IV q28d x 6 cycles) vs chlorambucil 0.4 mg/kg body weight (q15d x 12 mo) Overall survival, 46 mo vs 64 mo (p-value = 0.15) Eichhorst BF et al. Blood 2009;114(16):3382-91.
FC Improves Overall Survival in Non-High Risk CLL GCLLSG CLL4 protocol • 375 patients (<66 years) with advanced CLL were randomly assigned to fludarabine 25 mg/m2 x 5d IV q28d vs FC (fludarabine 30 mg/m2 and cyclophosphamide 250 mg/m2 x 3d IV q28d) • Complete remission rate, 24% vs 7% (p < 0.001) • Overall response rate, 94% vs 83% (p = 0.001) • Progression-free survival, 48 mo vs 20 mo (p = 0.001) • Treatment-free survival, 37 mo vs 25 mo (p < 0.001) Eichhorst BF et al. Blood 2006;107(3):885-91.
Improved Efficacy by Combining FC Chemotherapy with Rituximab (MD Anderson, historical comparison) p= 0.37 p< 0.001 F = fludarabine; M = mitoxantrone; C = cyclophosphamide; R-FC = fludarabine, cyclophosphamide and rituximab Tam CS et al. Blood 2008;112:975–80.
Median Progression-Free Survival N = 817 FCR, 57.9 mo vs FC, 32.9 mo Hazard ratio = 0.563 p < 0.0001 Hallek M et al. Lancet 2010;376:1164-74.
Median Overall Survival • 408 patients were assigned to fludarabine, cyclophosphamide and rituximab (FCR) and 409 patients to fludarabine and cyclophosphamide (FC) • FCR resulted in significant overall survival benefit: • FC, 48.4 mo vs FCR, 60.7 mo Hazard ratio = 0.75 p = 0.039 • At 4 years postrandomization: • 75.5% alive on the FC arm 81.8% alive on the FCR arm Hallek M et al. Lancet 2010;376:1164-74.
Overall Survival and Cytogenetic Abnormalities According to the Hierarchical Model FC FCR 3-yr OS* None: 86.9% 12q+: 85.8%11q-: 82.6% 13q-: 89.1% 17p-: 36.5% 3-yr OS* None: 83.8% 12q+: 95.8%11q-: 93.7% 13q-: 94.9% 17p-: 38.1% *p < 0.05 Hallek M et al. Lancet 2010;376:1164-74.
Bendamustine plus Rituximab Fischer et al, ASH 2009;Abstract 205. N = 110 (7 pts not yet evaluable)
Chlorambucil (Chl) plus Rituximab (R)in Older CLL Patients Hillmen et al, ASH 2010 Foa et al, ASH 2010 • CLB 8 mg/m2 d1-7 q28d up to 8x + R 375 mg/m2 c1-2, 500 mg/m2 c3-8, followed by R-maintenance 375 mg/m2 q 2 m for 2 yrs • CLB 10 mg/m2 d1-7 q28d up to 6x + R 375 mg/m2 c1, 500 mg/m2 c2-6 • CLB like B without R
CD20 Targeting Adapted from Lim et al, Haematologica 2010
CLL11 Protocolfor Unfit, Slow Go Patients Chlorambucil Chl Randomization Chlorambucilcombined withrituximab RChl Chlorambucil combined with GA101GChl
Third Generation of Trials of the GCLLSG: Risk, Stage and Fitness Adapted Inactive Binet A Active disease + all Binet C, not del(17p) CLL12 CLL10 CLL11 Which is the best score to define high risk? Go go Slow go no yes CLB CLB + R CLB + GA101 W&W W&W treat BR FCR Disease (MRD) eradication Longer survival Symptom control Longer disease-free survival
CD20 Targeting Adapted from Lim et al, Haematologica 2010
What is your usual preferred induction systemic regimen in a younger patient (60 years old) requiring treatment for CLL?
What is your usual preferred induction systemic regimen in an older patient (age 75) requiring treatment for CLL?
What Clinicians Want to KnowA Live CME Event Addressing the Most Common Questions and Controversies in the Current Clinical Management of Select Hematologic CancersSunday, June 5, 20117:00 PM – 9:30 PMChicago, Illinois Moderator Neil Love, MD Faculty Sergio Giralt, MDJohn P Leonard, MD Lauren C Pinter-Brown, MD Antonio Palumbo, MDSusan M O’Brien, MDProfessor Michael Hallek