Download
1 / 41
430 likes | 609 Views
Epidemiology and risk factors for breast cancer. Dr.Mina Tajvidi oncologist. Epidemiology and risk factors for breast cancer.

E N D
Epidemiology and risk factors for breast cancer Dr.MinaTajvidi oncologist
Epidemiology and risk factors for breast cancer In the US, breast cancer is the most common female cancer, the second most common cause of cancer death in women, and the main cause of death in women ages 40 to 59. About one-half of cases can be explained by known risk factors
Epidemiology and risk factors for breast cancer Incidence — Approximately 210,000 new cases of invasive breast cancer are expected to be diagnosed in the United States in 2010, and 40,000 die from the disease [1]. The lifetime probability of developing breast cancer is one in six overall (one in eight for invasive disease) Global variation — Globally, breast cancer incidence rates are highest in North America and northern Europe, and lowest in Asia and Africa
Age and gender Age and gender are among the strongest risk factors for breast cancer Breast cancer occurs 100 times more frequently in women than in men Incidence rates rise sharply with age until about the age of 45 to 50 when the rise is less steep
BENIGN BREAST DISEASE Single nonproliferative lesions (fibrocystic change, solitary papilloma, simple fibroadenoma) are not associated with an increased risk for breast cancer. The presence of multiple nonproliferative lesions may increase the risk for breast cancer modestly The more important precursors of noninvasive or invasive breast cancer are proliferative lesions, particularly those with cytologicatypia.
PERSONAL HISTORY OF BREAST CANCER A personal history of invasive or in situ breast cancer increases the risk of developing an invasive breast cancer in the contralateral breast
Weight Weight and body mass index (BMI) have opposite influences on postmenopausal as compared to premenopausal breast cancer. Higher weight/BMI and postmenopausal weight gain have been associated with a higher risk of breast cancer in multiple studies [34-39]. The influence of weight is strongest in women who do not use HT mean serum estradiol levels were significantly higher among women with a BMI ≥29 kg/m2 compared to those with a BMI <21 kg/m2 (10 versus 4.7 pg/mL) premenopausal women with a BMI ≥31 kg/m2 were 46 percent less likely to develop breast cancer than those with a BMI <21 kg/m2
Height In the majority of studies, increased height has been associated with a higher risk of both premenopausal and postmenopausal breast cancer women who were at least 175 cm (69 inches) tall were 20 percent more likely to develop breast cancer than those less than 160 cm (63 inches) tall
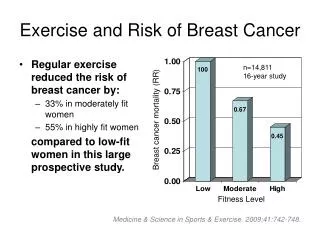
Physical activity Regular physical exercise appears to provide modest protection against breast cancer
Alcohol breast cancer risk is higher for women consuming moderate to high levels of alcohol
Fat intake Animal and ecologic studies have shown a positive correlation between fat consumption and increased breast cancer risk
Calcium/vitamin D inverse association between breast cancer risk and the intake of low-fat dairy products, calcium (mainly dairy intake), and vitamin D (mainly non-dairy intake) in premenopausal but not postmenopausal women
Antioxidants There is no strong evidence for an effect of intake of vitamin E, or C or beta-carotene on breast cancer risk [94,95]. The data are conflicting on vitamin A and breast cancer.
Smoking many showing modestly increased risk
REPRODUCTIVE/HORMONAL RISK FACTORS Prolonged exposure to and higher concentrations of endogenous estrogen increases the risk of breast cancer.
Age at menarche and menopause Younger age at menarche is associated with a higher risk of breast cancer Later menopause increases breast cancer risk
Menstrual patterns/infertility These events affect the number of lifetime ovulatory cycles and influence a woman's cumulative exposure to ovarian hormones. several epidemiologic studies suggest a link between infertility due to anovulatory disorders and a decreased risk of breast cancer
Parity Nulliparous women are at increased risk for breast cancer compared with parous women The protective effect of pregnancy is not seen until after 10 years following delivery
Age at first birth the cumulative incidence of breast cancer up to age 70 for parous versus nulliparous women was 20 percent lower if the first birth was at age 20, 10 percent lower for first birth at age 25, and 5 percent higher if the first birth was at age 35
Abortion ?????????????????
Breastfeeding A protective effect of breastfeeding has been shown in multiple case-control and cohort studies The protective effect of breastfeeding may be stronger for the development of breast cancer during the premenopausal years and in women with a first-degree relative with breast cancer
Bone density women with higher bone density had a higher breast cancer risk Because bone contains estrogen receptors and is highly sensitive to circulating estrogen levels
diabetes Although some studies suggest a slightly increased risk of breast cancer in postmenopausal women with type 2 diabetes [152-156], others do not [157-160]. Diabetes is not generally considered a significant breast cancer risk factor
Breast density Besides increasing the difficulty of mammographic detection, the presence of dense breast tissue is also independently associated with an increased risk of breast cancer In multiple independent epidemiologic studies, the risk of breast cancer is four to five times greater in women with mammographically dense breasts (usually defined as ≥75 percent density) compared to women of similar age with less or no dense tissue Breast density and bone mineral density are both markers for cumulative exposure to estrogen.
Oral contraceptives Many epidemiologic studies have failed to demonstrate an association between oral contraceptive use and the risk of breast cancer.
Hormone therapy The use of combined estrogen plus progesterone is associated with an increased relative risk of breast cancer; Long-term use of HT is associated with the highest risk. In contrast, short-term HT appears not to increase the risk of breast cancer significantly, although it may make mammographic detection more difficult.
Infertility treatment There does not appear to be an increased risk of breast cancer in women treated with fertility drugs. Further investigation is required.
FAMILY HISTORY AND GENETIC RISK FACTORS Family history is an important risk factor for breast cancer. However, a positive family history is only reported by 15 to 20 percent of women with breast cancer. the risk of breast cancer before age 40 was increased 5.7-fold if one relative had breast cancer before age 40. 5 to 6 percent of all breast cancers are directly attributable to inheritance of a breast cancer susceptibility gene such as BRCA1, BRCA2, p53, ATM, and PTEN
EXPOSURE TO IONIZING RADIATION Exposure to ionizing radiation of the chest at a young age, as occurs with treatment of Hodgkin lymphoma or in survivors of atomic bomb or nuclear plant accidents, is associated with an increased risk of breast cance The most vulnerable ages appear to be between 10 to 14 (the prepubertal years), but excess risk is seen in women exposed as late as 45 years of age [191]. After age 45, there does not appear to be any increased risk mammography, chest radiographs, diagnostic spine imaging [192,193], CT scans), is controversial. At least for women without an inherited predisposition to breast cancer, the impact of radiation-associated breast cancer from routine diagnostic imaging is thought to be small to nonexistent
ENVIRONMENTAL EXPOSURES Organochlorines include polychlorinated biphenyls (PCB's), dioxins, and organochlorine pesticides such as DDT. These compounds are weak estrogens, highly lipophilic, and capable of persisting in body tissues for years. However, most large studies have failed to find an association Cosmetic breast implants, electromagnetic fields, electric blankets, and hair dyes have not been associated with increased risk in most studies
Nocturnal light exposure/Night shift work At least three studies and a meta-analysis support an association between exposure to light at night and the risk of breast cancer
NSAID use Aspirin and other nonsteroidalantiinflammatory drugs (NSAIDs) can inhibit the formation of both benign and malignant tumors in the colon. the data regarding a possible protective effect of NSAID ingestion on breast cancer risk are mixed. Only one randomized trial has evaluated the impact of low-dose aspirin on cancer prevention
Antibiotic use increasing cumulative days of antibiotic use for any condition was associated with a significantly greater risk of breast cancer. they underscore the importance of carefully considering the use of antibiotics in the absence of a clear indication.
Screening for breast cancer A variety of imaging modalities have been developed for identifying lesions that are suspicious for breast cancer. Mammography remains the mainstay of screening for breast cancer
Mammography digital mammography was more accurate for premenopausal and perimenopausal women, and for women with dense breasts film mammography remains an acceptable screening modality for all women. Digital mammography, when available, may offer a small screening advantage in women younger than 50 years old.
Magnetic resonance imaging The combination of MRI and mammography is recommended by the American Cancer Society in women at very high risk of breast cancer Nearly all invasive breast carcinomas enhance on gadolinium contrast-enhanced MRI The reported sensitivity of breast MRI is 88 to 100 percent for invasive carcinomas; it is lower for DCIS in most, but not all
Age to initiate screening The American Academy of Family Physicians recommends screening mammography every one to two years for women ages 40 and older Age to discontinue :age 74.