Download
1 / 64
640 likes | 924 Views
Diastolic LV function and HFNEF. FRIJO JOSE A. Approximately 50% of pts with HF have a normal or near normal LVEF Mayo Clinic registry. Women Hypertension (up to 88%) Obesity (BMI >30 kg/m2 → 40%) Renal failure Anemia AF Diabetes (30%) CAD (40%-50%)

E N D
Diastolic LV function and HFNEF FRIJO JOSE A
Approximately 50% of pts with HF have a normal or near normal LVEF Mayo Clinic registry
Women • Hypertension (up to 88%) • Obesity (BMI >30 kg/m2 → 40%) • Renal failure • Anemia • AF • Diabetes (30%) • CAD (40%-50%) similar to that in HF patients with impaired LVEF
Lower overall mortality in HFNEF v/s SHF patients (2.8% vs 3.9%; P = 0.005) • Symptom burden, duration of ICU stay & hospital stay, long-term mortality – similar ADHERE database- 52,187 patients
Clinical ∆ of HF (Framingham criteria) and an LVEF > 50% • True- typically excluded • “significant”CAD(most often clinically assessed) • Hypertrophic cardiomyopathy • Valvular heart disease
Morphologic Features • Higher cardiomyocytediameter • Higher myofibrillar density • Collagen volume fraction was similar
Diastolic function • Major factors influencing relaxation • Cytosolic Ca level must fall- requires ATP & phosphorylation of phospholamban • Inherent viscoelastic properties of myocard – (hypertrophied heart -↑fibrosis, relaxation –slower) • ↑phosphorylation of troponin I • Influenced by systolic load- ↑the systolic load, the faster the rate of relaxation
Diastolic function • SHF pts →LV pressure–volume analysis →less steep slope of end-systolic LV pressure–volume relationship • HFNEF pts → • Upward and leftward shifted end-diastolic pressure–volume relationship • End-systolic pressure–volume relationship- unaltered or even steeper
HFNEF • ↑LV stiffness • Very small changes in LVEDV→ Marked ↑ in LVEDP & pulm venous P→ dyspneaduring exercise, even pulmedema • Impaired LV filling and inability to use Frank-Starling mech→ Failure to ↑CO during exercise→ Exercise intolerance
Is diastolic dysfunction the only explanation? • TDI - ↓ systolic mitral annular amplitudes—in HFNEF pts V/S controls • These changes – not as pronouncdas in SHF pts • ?initial abn compensated for by ventrihypertrophy & neurohormonal activation →hypercontractileLV state with abn relaxation →resistance to LV filling →progress →phenotype characteristic of SHF • However, data lacking & progression have been shown to occur rarely
2,042 participants • Incidence of mod-sevLV diastdysf in presence of an LVEF >50% - 5.6% • Only ~ 1%of study population had symptoms of HF & an LVEF >50%. Redfield MM et al. JAMA 2003;289:194 –202.
37 HFNEF pts (prevpulmedema, LVEF >50%) • 40 pts with hypertensive LVH without HF • 56 control subjects • HFNEF V/S HTN LVH and control - ↑LV mass index, ↑concLV geometry, ↑E/E’ratio, ↑LA volume • Distinguished HFNEF pts very well from control but not from asymptomatic hypertensive LVH • Product of LV mass index and LA volume -highest accuracy for predicting HFNEF MelenovskyV et al. J Am Coll Cardiol2007;49:198–207
Anemia, renal dysf • ? Volume overload rather than an intrinsic abnof LV diastolic function -pathophysio of HFNEF
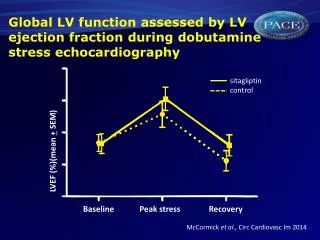
LV systolic function • LVEF as a measure of LV systolic function -questioned-load dependence • Annular peak syst velocity (TDI) ↓in HFNEF • Still controversial- whether LV syst function is N in HFNEF
Ventriculovascular coupling in HFNEF • Effective art elastance- global measure of art stiffness-(LVESP/SV)- ↑ HFNEF pts • Combined ventri-art stiffening contributes to HFNEF Mechanisms • 1) exaggerated↑ SBP after small ↑ in LVEDV • 2) a marked ↑ SBP after a further ↑ in art elastance in presence of a high ES elastance • 3) limited systolic reserve due to ↑ baseline ES elastance • 4) ↑ cardiac work to deliver a given CO • 5) a direct influence of ↑ art elastance on LV diast functn First 2 also explain sensitivity of these pts to overdiuresis & aggr vasodilator therapy
Role of Atrial Fibrillation Atria • Blood-receiving reservoir chamber • Contractile chamber • Conduit • Volume sensor of the heart, releasing ANP in response to intermittent stretch • Contains receptors for afferent arms of various reflexes • mechanoreceptors that ↑sinus discharge rate, thereby contributing to the tachycardia of exercise as the venous return increases (Bainbridge reflex)
Role of Atrial Fibrillation • The prevalence of AF in HFNEF ≈ 20% to 30%
Fung et al- HFNEF pts with AF (29%) had ↓functional class & quality of life than without AF • CHARM - AF →adv CV outcomes irrespective of baseline LVEF • High HR, loss of atrial systole, irr cycle length with implications of the Frank-Starling mechanism, episodic nature • Echocardiographic assess challenging • Fung et al - similar E/E’ ratios in HFNEF with and without AF but larger LA size in AF • Melenovsky et al - LA emptying fraction ↓in HFNEF pts than hypertensive LVH & during handgrip, late diastolic annular tissue velocity - unchanged in HFNEF but ↑ in control (5% vs. 35%)
Role of Coronary Artery Disease • Ischemia affects early diastole by ↑ Tau • Reversed after removal of ischemic burden by CABG • ?Considerable no of pts with atypical presentation of ischemia (silent/dyspnea) labeled as HFNEF • 15% incidence of hospital admission due to UA in pts previously ∆ with HFNEF -38/12
Volume overload • HF with either ↓/NEF is a Na-sensitive condition • HFNEF- ↑ likely to have multiple comorbidities that may contribute to volume overload • Renovascular disease, obesity, OSAHS, anemia • Plasma volumes of HTN HFNEF - ↑ by an average of 16% compared with N controls despite daily diuretic use
UNLOAD -ultrafiltration -186 pts -45 NEF→½ ultrafiltration, other ½ IV diuretics • Volume expansion precedes sympt, volume removal alleviates sympt without inducing hypotension/end-organ dysf • HFNEF → ↑ risk of recur of fluid overload • A/c pulm edema - common manifestation of HFNEF→ diuretics remain mainstay • Diuretics & dietary salt restrict- paramount to care of HFNEF pts
Venoconstriction/volume redistribution • ≈ 85% of blood vol- venous circulation • Small alterations in venous tone & capacitance (esp splanchnic bed) → impact the distri of intravasc vol - imp determinant of LVED filling P • Data lacking • Most imp drugs used in a/c pulm edema → venodilators & diuretics ? Improvements-at least partly due to ↓autonomic tone & resulting ↑in venous capacitance
Diagnosis of HFNEF 2007- European Working Group on HFNEF 3 conditions must be fulfilled • 1) symptoms & signs of HF • 2) LVEF >50% in a nondilated LV (LVEDV<97 ml/m2) • 3) evidence of ↑LV filling P 3 ways to ∆ ↑ LV filling P • invasive measurements • unequivocal TDI findings • combination of ↑natriuretic peptides & echo indices of LV diastolic function/LV filling P Paulus Wjet al -European Society of Cardiology. Eur Heart J 2007;28:2539 –50
Invasive Diagnostics • Prolonged & ↑ Tau- require sophist measurement • ↑ LVEDP /PCWP - suggested to be appropriate for ∆ of HFNEF in the presence of HF sympts & LVEF>50%
The rate of isovolumic relaxation - best measured by negative dP/dtmax at invasive catheterization • The -dP/dtmax, which gives the isovolumic relaxation rate- measured either invasively or by a CW Doppler velocity spectrum in AR • Isovolumic relaxation is ↑when rate of Ca uptake into the sarcoplasmic reticulum (SR) is ↑ • Tau- time constant of relaxation- describes rate of fall of LV pressure during isovolumic relaxation -also req invasive for precise determination
Isovolumic pressure decay • Simplest way of quantifying the time course of LV pressure decline - peak -dp/dt • Peak -dp/dt - altered by myo relaxation & changes in loading conditions • For eg, LV peak -dp/dt ↑ when Ao pressure ↑ - ie, ↑ in LV peak -dp/dt from -1,500 to -1,800 mm Hg/sec could be caused by an ↑ in rate of myo relaxation, a rise in Ao pressure, or both • LV peak -dp/dt is ↓during myo ischemia & is ↑ in response to – β adr stimulation & phosphodiesterase inhibitor milrinone • It is not↑ by digitalis glycosides
Echocardiography • Currently most sensitive & widely available technique for assessment of LV diastolic function –TDI • Whereas the ratio of early to late diastolic peak mitral inflow velocities exhibits a J-shaped relationship with LVEDP, TDI velocities continuously decline from N to advanced LV diastolic dysfunction • As a consequence, E’ ↓ & E/E’ ratio continuously ↑with advanced LV diastolic dysfunction
E/E ’ ratio >15 → mean diastolic LV pressure >12 mm Hg • E/E ’ ratio >15 - ∆ of ↑ LV filling pressure and thus HFNEF • An E/E ’ ratio 8 – 15- asso with very wide range of mean LV diastolic pressures, thus, further measurements suggested
Values for E ’ at the lateral annulus are generally higher than at medial annulus, resulting in lower E/E ’ ratios at the lateral annulus
Grade 1 Grade 2 Grade 3 Grade 4 LVpressure Diastolic Dysfunction E Mitral flow TissueDoppler e’ Pulmonaryvein E/e’ < 10 10 -15 >15 >15
Mitral E Annulus e E/e As LV fillingpressure Nagueh et al: JACC, 1997 Ommen et al: Circ, 2000
Measurement of velocity of mitral annular ascent during early diastole (e′vel) with TDI → relatively preload-independent measure of LV relaxation that correlates inversely with tau • E/e′ ratio is a fairly accurate predictor of the presence of elevated filling pressures
Area-length method for calculation of LV mass LVmass=1.05[5/6(A1xL1)-5/6(A2xL2)] Divide by body surface area to get LV mass index Reichek et al. Circulation 1983;67:348-52