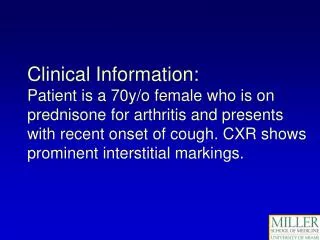
Download
1 / 27
320 likes | 694 Views
Tibion Bionic Leg: Application to the neurologic Patient. Jenny Wang, PT, DPT, MS Swedish Medical Center Englewood, CO. Objectives . Discuss how robotics can enhance training, learning, and rehabilitation goals. Selecting appropriate patients and outcome measures. Rehabilitation Robotics.

E N D
Tibion Bionic Leg: Application to the neurologic Patient Jenny Wang, PT, DPT, MS Swedish Medical Center Englewood, CO
Objectives • Discuss how robotics can enhance training, learning, and rehabilitation goals. • Selecting appropriate patients and outcome measures.
Rehabilitation Robotics • Class of robots that can integrated into rehabilitation programs at home, in health care settings, at work, or in the community to enhance function. • Integrated as a tool to enhance the effectiveness of one on one therapy to promote recovery, independence, and maximal function.
Rehabilitation Robotics • Learning based robotic systems include virtual reality, games for memory, and technology to improve physical performance • Enables patient to perform quality controlled, repetitive, progressive, task- oriented practice to improve learning • Bioness systems • Tibion Bionic leg
Assistive Robotics • Can be classified as non-wearable or wear-able
Tibion Bionic leg Robotic exoskeleton placed on patient’s leg during training.
Tibion system • Provides mechanized assistance for patient initiated active movement • Flexible plantar pressure-sensing shoe insert • Loose fitting plastic ankle straps attaching the shoe insert without providing ankle support • Leg and thigh uprights • Single axis knee joint with angle sensors • Textile straps secured with zippers • Velcro and adjusting knobs • Onboard actuator motors with control panel housing • Rechargeable lithium battery
Tibion • Plantar pressure sensors detect gait phases through weight bearing • Angle sensors detect knee motion angles • Actuator torque sensors determine knee torque
Application in rehab • Maximizes neural plasticity and recovery of motor control, sensation, and physical skills through controlled, progressive repetition • Improves endurance, quality of movement, more complete task performance, independence, and quality of life • Task specific training focused on functional tasks like transfers, gait training, and stairs
in motion • During stance phase, stair climbing, and sit>stand movements, knee actuator assists knee concentric extension. • During toe off and non-weight bearing conditions, actuator decouples and allows for free knee swing. • Patient initiated knee extension with weight bearing triggers mechanically assisted knee extension based on programming. • Resistance and timing parameters can be set by P.T. based on patient performance.
parameters • Weight: 110-300 lbs. • Start force: weight on foot plate required to initiate powered assist • Assist factor: amount of knee extension assistance provided (concentric) • Resist factor: amount of knee extension assistance provided during flexion (eccentric) • Assist extension limit: degree of extension through which assistance is provided. Helps limit knee hyperextension when present
Swedish rehab • Patient population: • Comprehensive Rehab unit (amputees, orthopedics/multi-trauma) • CVA* • Brain tumors • SCI • TBI • MS • PD
Patient selection • Patient motivation • Physical/cognitive ability to use and follow multi-step directions • Height • Stroke patients with the most consistent outcomes
Patient case • 59 yo female • Medical history: L pontine and cerebellar ischemic infarcts, basilar artery thrombosis s/p TNK and stent angioplasty • Past medical history: R femur fracture s/p IM nailing from auto accident 30 yrs ago, dyslipidemia, pre-HTN, migraines • Premorbid functional status: Independent with functional mobility and ADLs, working full time as dental assistant • Discharged from rehab unit after 4 weeks with supervision/assistance from family
Patient case • Impairments: Mobility and Strength • Bed mobility: Minimal assistance • Transfers: Minimal-Moderate assistance • Gait: Ambulate 2 steps forward w/out UE support, Min-Max Assist for balance and R foot placement. Trendelenburg and Genu Recurvatum on RLE. • Right leg strength • Hip flexion 2-/5 • Knee flexion 2-/5 • Knee extension 2-/5 • Dorsiflexion 0/5
Outcomes • Functional status: bed mobility, transfers, gait, stairs • Five time sit to stand • Body structure and function Domain of ICF model of disability • Measures: • Lower limb strength and function • Balance and mobility • Predictor of recurrent falls • General test of physical performance • Correlates with DGI, TUG, Gait speed, BBS
outcomes • Gait speed • Activity Domain • Measures: • Motor control • Muscle performance • Endurance and activity level • Musculoskeletal condition • Correlates with discharge location, additional need for rehabilitation, functional status • Indicator for household ambulator, limited community ambulator, or community ambulator
Treatment paradigm • Projected functional goals at discharge established at initial evaluation • Bed mobility • Transfers • Gait • Stairs • Initial treatment aimed at quality of movement ie. trunk control, hip stability, midline orientation, safety with mobility, and lower extremity activation.
Treatment paradigm • Based on principles of motor control and learning, performed function based training using Tibion Bionic leg initially for standing weight shifting, sit><stand, then gait. • Tibion initiated on Day 9 for gait training, after interventions addressing safety, midline orientation, knee control, appropriate hip stability, and trunk control/alignment. • Continual intervention for functional mobility in conjunction with use of Tibion and Bioness L300. • Also participating in 1.5 hrs of OT and 1 hr of SLP services
Summary • Challenges: • Not available for personal rental for home use • Difficult fit for smaller stature/petite patients