Download

1 / 66
660 likes | 795 Views
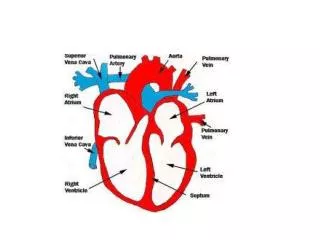
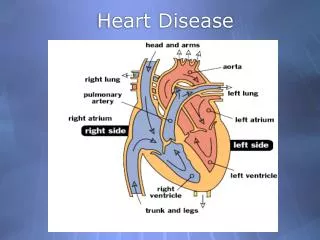
New Trends in Heart Disease. Prof Chu-Pak Lau Cardiology Division University of Hong Kong Queen Mary Hospital. Public Health Conference 6 March 2004. Global Burden of CVS disease Bonow RO et al Circ 2002; 106:1602-1605. CVS death toll : 14.7M in 1990 to 17M 1999

E N D
New Trends in Heart Disease Prof Chu-Pak Lau Cardiology Division University of Hong Kong Queen Mary Hospital Public Health Conference 6 March 2004
Global Burden of CVS diseaseBonow RO et al Circ 2002; 106:1602-1605 • CVS death toll : 14.7M in 1990 to 17M 1999 • Main burden due to CAD, is the leading cause of death worldwide (30%). CVA second leading cause • WHO : 1 Billion people overweight 18M children <5 are overweight • 60% of the world population is physically inactive • DM : 150M people, will double in 2025 • Tobacco consumption still increasing
Coronary Artery Disease Heart Failure Atrial Fibrillation
CVS Death per 100,00 population AHA Heart & Stroke Statistics 1999 Men Women
Sino-MONICA Project.Circulation 2001; 103:462-468(1) • 7 Year project (1987-1993) • WHO project • Collaboration with BIHLBD
Sino-MONICA Project.Circulation 2001; 103:462-468(2) • Incidence and mortality of CVS disease is low but those of CVA were high • Great disparity in incidence CVS : 108.7/100,000 to 3.3/100,000 for men CVA : 553.3/100,000 to 33/100,000 3. Geographical difference : North > South e.g. Beijing 70.3 vs Guangdong 59.7/100,000
Leading Causes of Death in US and HK (Female) Year 2000 Per 100,000 population
Special Features of Heart Disease of Women • Older • Delayed presentation • Higher mortality rate • Triple vessel disease and smaller vessel size • Higher CABG risk • Suboptimal response to PTCA • Despite a lower CAD risk, HK women have mortality from strokes comparable to the US
Modifiable Risk Factors Hypertension Hypercholesterolemia Diabetes mellitus Homocysteine C-Reactive Protein Exercise Obesity Cigarette smoking
BP, Cholesterol and Stroke in Eastern Asia Eastern Stroke and Coronary Heart Disease Collaborative Research Group Lancet 1998; 352; 1801-1807
Obesity Prevalence in the US in American white (1999-2000) Obesity : BMI > 30 CDC 1999-2000
Mortality from CAD in HK (Dept of Health Annual Report 1997-2001) (1) No. of Pts
Mortality from CAD in HK (<45yrs)(Dept of Health Annual Report 1997-2001) (2) % of Heath Disease <45 years %
The Role of Platelets in Inflammation and Plaque Stability Activated platelets Inflammatory modulators CD40L Platelet-derived growth factor Platelet factor 4 RANTES Thrombospondin Transforming growth factor- Nitric Oxide Plaque rupture & thrombosis Libby P. Circulation 2001:103:1718-1720
Lipoprotein(a) Homocysteine VCAM-1 Fibrinogen LDL-C ICAM-1 hs-CRP TC:HDL-C CRP + TC: HDL-C 0 1.0 2.0 4.0 6.0 Novel Risk Factors as Predictors of Peripheral Arterial Disease Relative Risk of Incident Peripheral Arterial Disease (Adjusted for age, smoking, DM, HTN, family history, exercise level, and BMI) Ridker et al. JAMA 2001;285:2481-2485
AHA/CDC Recommendations for Clinical and Public Health Practice Clinical Practice • Measurement of hs-CRP is an independent marker of risk and, in those judged at intermediate risk by global risk assessment (10%-20% CHD/10 yr) may help direct further evaluation & therapy in primary prevention of CHD. The benefits of such therapy based on this strategy remain uncertain. (Class IIa, Level of Evidence B) • Measurement of hs-CRP may be used at discretion of the physician as part of global risk assessment in adults without known CVD. The benefits of such therapy based on this strategy remain uncertain. (Class IIb, Level of Evidence C) AHA/CDC Statement. Circulation 2003; 107:499–511
Hong Kong Cardiovascular Risk Factor Prevalence Study-2 (CRISPS2) Bernard Cheung Department of Medicine University of Hong Kong
Weight • Body weight increased by 0.54±0.14 kg (p<0.001) • There was no significant change in body mass index (BMI) • Waist circumference increasedfrom 78.3±0.3 to 80.5±0.3 cm (p<0.001)
Prevalence of overweight and obesity in the study population
BMI25 is associated with diabetes (OR 3.1 [2.0-4.7]) and hypertension (OR 3.5 [2.5-5.0]) Overweight, diabetes and hypertension
Conclusions • In the CRIPS2 cohort, hypertension (27%), diabetes (15%), hypercholesterolaemia (46%) and overweight (35%) are common • As these risk factors can be modified by diet and lifestyle, the prevention of cardiovascular disease requires a community approach
Coronary Artery Disease • Heart Failure Atrial Fibrillation
Heart Failure : How Big is the Problem Really? • 4,790,000 Americans have heart failure • Based on extrapolation of NHANES data • 550,000 new cases each year • Based on extrapolation of 44-year Framingham data • HF contributed to 287,200 deaths in 1999 • Primary cause in 54,913 • HF deaths have increased by 145% in 20years • Age-adjusted rates have not changed • Mortality rates may be declining • Hospital discharges increased from 377,000 to 962,000 between 1979 and 1999 • Age adjusted rates and length of stay are declining
65+ 45-64
A New Epidemiology of Ventricular Dysfunction The Old Epidemiology of CHF : • Included only symptomatic LV failure • Often excluded persons > 75 years old • Did not characterize ventricular function The New Epidemiology of Ventricular Dysfunction : • Includes assessment of ventricular structure and systolic / diastolic function • No age limits
Community Echo Survey of Systolic and Diastolic LV DysfunctionRedfield MM et al, JAMA 2003; 289: 194-202 Pts & Methods 1997-2000 : 2042 subjects of Olmsted County were screened with echo and Doppler, and followed for ~5yrs Results CHF : 2.2% Systolic Dysfunction : 6% EF > 50% : 44% Diastolic Dysfu : Mild 20.6% Mod 6.6% Severe 0.7%
Pharmacotherapy • ACEI • Angiotensin II blockers • Betablockers • Aldosterone antagonist • Newer agents
Declining Mortality in Heart Failure Trial Severe Mild-Mod
Prevalence of Heart Failure with Preserved EF EF> 45% EF> 50% N=269 EF> 45% N=338 EF> 40% N=782 EF> 50% N=137 EF> 50% N=73
Main Problems of Electrical Alterations 1. PR prolongation (improper LV filling) 2. Interventricular asynchrony (RV-LV asynchrony) 3. Intraventricular asynchrony (regional LV asynchrony) Results in : 1. Stroke volume 2. Contractility 3. MR
Before After CRT or Reverse Remodelling ?
CRT Trials 6m HW (m) Echo (LVED in mm) LVEF (%) *Significant Improvement
COMPANION : Death or HF Hospitalization(% of composite Endpoints) Bristow MR ACC 2003
Coronary Artery Disease Heart Failure • Atrial Fibrillation
AF : Incidence/resource implication In USA : 2 million; 160,000 new cases/yr 3-5% population >60yr 1.5 million primary reasons for consultation 1.4 million hospital discharges 130,000 A&E visits 6.6 billion US$ Medicare