Download
1 / 28
280 likes | 1.31k Views
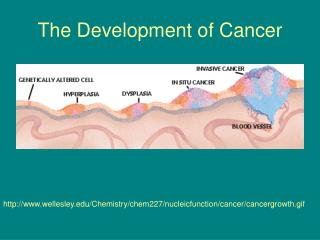
Cancer of The Vulva. By Dr Emdalala Elasheg. Introduction Vulval cancer is uncommon and accounts for approximately 1-4% of all gynecological cancer

E N D
Cancer of The Vulva By Dr Emdalala Elasheg
Introduction • Vulval cancer is uncommon and accounts for approximately 1-4% of all gynecological cancer • incidence : 1.8 /100.000, It is predominantly seen in postmenopausal and old women (mean age 65 years ) ,and only 2% were less than 30 years. • In countries such as south Africa where sexually transmitted diseases are common, the mean age of presentation is 59 years.
Objectives • To know the out lines of etiology,diagnosis and mangment of cancer vulva. • To understand the importance of early dectection of cancer vulva to improve prognosis and survival rate
AETHIOLOGY: Little is known • A viral factor has been suggested by the detection of antigens induced by • Herpes simplex virus type (HSV2) • Type 16/18 human papilloma virus (HPV) , in vulval intraepithelial neoplasia.
PATHOLOGY Primary Tumor • 90% of lesions are of squamous in origin. • 3-5 of lesions are melanoma. • 2% of lesions is basal cell carcinoma. • Less than 1% is sarcoma. Secondary Tumors • It is occasionly found in vulva Most commonly the primary lesion is from the cervix or the endometrium .
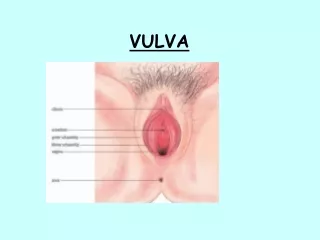
SQUAMOUS CELL CARCINOMA • Are usually seen in the anterior part of the vulva. • 2/3 of cases in the labia majora. • 1/3 of cases in the clitoris ,labia minora,fourchitte, and perineum. Spread:- • LYMPHATIC > 50% • Direct spread occurs in 25% to the urethra, vagina and rectum • Hematogenous spread to bone or lung is rare The lymph nodes are arranged in 5 groups in each groin:
Superficial L.N: 1- Inguinal L.N: Medial I.L.N ,lying inferior to S.I.ring. Lateral I.L.N ,below the inguinal ligament. 2-Femoral L.N: Medical F.L.N,lying medical to saph.vein Lateral F.L.N, lying lateral to saph .vein
Deep L.N: • Deep inguinal L.N , lying in the inguinal channel • Deep femoral L.N (node of cloquet lying in the femoral channel • External iliac L.N: Medial groups ,lying medial to EIV Lateral groups,lying lateral to EIA Anterior groups ,lying between EIV and EIA
External Iliac Nodes Common Iliac Nodes Thoracic Duct Para Aortic L.N • Lt sided lesion will spread to the Lt groin Lymph node. • Rt sided lesion will spread to the Rt Groin Lymph node. • Bilateral nodes involvement is seen in 14% of cases. • Contralateral node involvement without ipsilateral disease is seen in 5% of cases. • Never found pelvic nodes to be involved in the absence of inguinal nodes metastases.
Clinical Features & Diagnosis Most patients with invasive disease complain of: • Irritation or purities in 70% of cases • Vulvar mass or ulcer in 55% of cases • Bleeding in 28% of cases • Discharge in 2-3% of cases
The major problem in invasive vulvar cancer is delay between the first appearance of the symptoms and referral to the gynecological opinion due to : • The doctor fails to recognize the gravity of the lesion and prescribes topical therapy. • Older women are often embarrassed and shy.
On Examination • Lesion can take any form from flat white lesion to large ulcer.the size of the tumor ,involvement of the urethra and anus should be noted • Inspection of the cervix and cervical cytology. • Needle aspiration of any suspicious groin node. diagnosis is made on histology from full thickness generous biopsy.
STAGING: FIGO suggest clinical staging in 1969 based on TNM (Tumor node metastasis) classification taking into consideration: • The size of the local lesion. • Groin node involvement. • Metastases.
A new FIGO staging based on surgical findings in 1988, it is more accurate as the involvement of groin nodes is missed on clinical examination in up to 30% of cases and over diagnosis in 5%.
PROGNOSIS The overall 5 years survival rate for vulval cancer is 70% for all operable cases, This depends on: • L.N Involvement: • This is the most prognostic factor • Metstatic involvement of groin nodes decreases the 5 years survival rate to below 50% as opposed to the 90% when L.N are not involved. • Once pelvic nodes are involved the 5 years survival rate is 15%.
The number of groin nodes involvement: • microscopical involvement of N.regardless of stage has a good prognosis. • 2 or more positive nodes have a worse prognosis. • Stage: • The 5 years survival rate decreases with advancing stage from >90% in stage 1 to < 10% in stage 4. • Differentiation: • A well diff.tumor has a better prognosis than poor diff.
Depth of Invasion: A-invasion of 1 mm no risk of nodal metastases. B-invasion of 1-3 mm 6-8% incidence of metastases. C-invasion of 5 mm 22-37% incidence of metastases. • Surgical Margin: Surgical excision margin of more than 1 cm in all diameters results in a low local recurrence rate.
Treatment • The corner stone of treatment is surgery • The majority of FIGO stage 1 and 2 will be cured by surgery alone. • Because most vulval cancers present at an advanced stage in developing countries other modalities such as chemotherapy and radiotherapy may have to be used.
SURGURY: • The standard surgery is enblock radical vulvectomy and bilateral groin nodes dissection as described by Taussing and way (three separate incision). This associated with: • High incidence of morbidity (wound infection, necrosis and break down , pul. Embolism, and lymphoedema). • Problems with bodyimage and sexual function.
The recent trend in management is not to cure patients but to preserve body image and sexual function by performing less radical surgery .The individualization of the treatment depends on: • Size and position of tumor. • Depth of invasion. • The age and performance status of the patient.
Nowadays they found that pelvic node radiation is better than pelvic node dissection because: PND (pelvic node dissection)PNR(pelvic node radiation) Survival rate 2 years 55% significant improvement of survival rate of 2 years 70%
CONCLUSION • Any patient with persistence itching or vulval lesion not responds to simple treatment , you should take multiple biopsies from vulva to exclude malignancy. • In management of cancer vulva, age group, psychology of patient, and the appearance of the vulva should be taken in account as this will change the plan of management of cancer. • Plastic surgery should play role in the future. • In future infrared , and laser therapy under microscopy will play role in the management of premalignant lesions.