Download
1 / 82
830 likes | 995 Views
World Bank Training Program on HIV/AIDS Drugs Training Module 4 Quality Assurance Ben K Botwe April 2005. Learning Objectives. Upon completion of this module, you will be able to. Explain the need for a systematic quality assurance process for pharmaceutical products

E N D
World Bank Training Program on HIV/AIDS DrugsTraining Module 4Quality Assurance Ben K BotweApril 2005
Learning Objectives Upon completion of this module, you will be able to • Explain the need for a systematic quality assurance process for pharmaceutical products • Describe key elements of the quality assurance process for pharmaceuticals • Discuss the procedures and standards for prequalification of suppliers of pharmaceuticals • Apply quality assurance and supplier selection principles to case discussions
Rationale for this Module • Quality medicines are safe, effective and efficient tools for treatment of HIV/AIDS • Poor quality (sub-standard) medicines may not produce desired effects, may cause harm • Errors in production can lead to sub-standard medicines • Quality Assurance principles can be used to detect errors or problems in production and ensure suppliers conform to standards and expectations • Battling HIV/AIDS: A decision maker’s guide to the procurement of medicines and related supplies provides framework for quality assurance
Outline of the Presentation • Introduction, Definitions and Quality Assurance • Good Manufacturing Practices • Product Selection • Suppliers and Manufacturers • Selection and Sourcing • Procedures for Prequalification of Suppliers • Stability and Equivalence • Conclusion • Case Study
Quality Assurance • A process, not an end-point • Must be independent of financial pressures • Must ensure that quality policies are followed • Must have final authority in product acceptance, rejection and release to public • Integral to production, not an add-on • Responsible for day-to-day operations and for longer term goal settings • Quantitative discipline with specified parameters
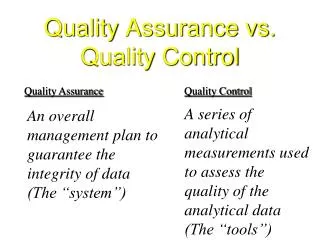
DEFINITIONS • QUALITY • The totality of features and characteristics of a medicinal product and its ability to satisfy stated and/or implied needs • QUALITY ASSURANCE • The sum total of the organized arrangements made with the object of ensuring that medicinal products are of the quality required for their intended use.
DEFINITIONS • GOOD MANUFACTURING PRACTICE (GMP) • That part of QA which ensures that products are consistently produced and controlled to the quality standardsappropriate to their intended use. • QUALITY CONTROL • That part of GMP which is concerned with sampling, specifications and testing.
Quality relationships QA GMP QC
Quality relationships Quality Management Quality Assurance GMP Quality Control
FACTORS IN DRUG QUALITY ASSURANCE IMPORT & EXPORT CONTROL LEGISLATIVE FRAMEWORK -REGULATIONS PACKAGING HUMAN RESOURCES- PROFESSIONALS LABELLING & PRODUCT INFROMATION DRUG PRODUCT QUALITY RAW MATERIALS- ACTIVE & INACTIVE QC & ANALYSIS TRANSPORT DISTRIBUTION DISPENSING & USE MANUFACURING PROCESSES & PROCEDURES STORAGE
Quality Assurance Primary Functions • Quality Control • Analytical testing of products • Active and Non active material control • Sampling, inspecting and testing of incoming raw materials • Packaging and labeling components • Bottles, caps, foils, labels, measures, cartons • Physical inspection of product and operations at critical intermediate stages • In-process controls, HHACCP • Control of product through its distribution • GSP, GDP ETC
Quality Must Be Designed Into A Product • Quality is not an add-on: it begins with research and development • Product quality criteria must be established • Detailed specifications provide quantitative parameters for measurement • Written procedures document how quality is attained and maintained • Continuous monitoring (sampling, testing) to confirm quality is being built-into product
Elements of the Quality Assurance Cycle in Pharmaceutical Manufacturing • Research • Development • Prototyping • Documentation • Raw Materials • Facilities • Equipment • Personnel and Supervision • Monitoring, Feedback, Follow-up
Analytical Control Laboratory Heart of Quality Management in Pharmaceuticals • Academically trained and certified staff • Experienced supervision/management • Capable of performing complex analyses • Able to report honestly and in a timely manner • Equipment and instrumentation must be suitable for performing testing • Access to reliable power, water and other stable infrastructure
Quality Control & Analysis • Qualification • Design, Installation, Process and Operational • Calibration • Daily and periodic • Validation • Equipment, Method and process • SOPs • Authorized, used and updated • Documentation • Systematic and well kept • Quality Manual • Quality manager, staff trained and motivated to comply. • Safety measures
Quality Assurance Throughout the Manufacturing Process • Monitoring environmental conditions under which products are manufactured/stored • Monitoring of air and water systems to prevent contamination– Air Handling Units • Monitoring of humidity • Monitoring of personnel • Feedback and follow-up
Manufacturing Process and Procedures • Dispensing / Weighing • Mixing / Granulation / Preparation • Compression / Encapsulation / Filling • Equipment, Operational & Process Qualification • Validation & calibration • Documentation and record keeping • Yield Reconciliation
A Guiding Philosophy for Quality Assurance in the Pharmaceutical Industry Poor Quality Medicines: • Are a health hazard • Waste money for governments and consumers • May contain toxic substances that have unpredictable, unintended consequences • Will not have a desired therapeutic effect • Does not save anyone any money in the long term • Hurt everyone – patients, health care workers, policy makers, regulators, manufacturers
CONSEQUENCES OF QA BREACHES • Poor Treatment outcomes • High Health Bills • Treatment Failures & Deaths • Loss of Confidence in the Health Services • Enormous Economic Losses • National Security Issue
What is GMP? (WHO) • Comprehensive system for ensuring products are consistently produced and controlled according to quality standards • Designed to minimize risks involved in any pharmaceutical production that cannot be eliminated through testing of final product alone • Cross-contamination
Major Risks in Pharmaceutical Production • Contamination of products (microbial, particulate or other) • Incorrect labels on containers • Insufficient active ingredient • Excess active ingredient • Poor quality raw materials • Poor formulation practices
Analysis of Substandard Medicines Source: (WHO)
The Breadth of GMP Covers all aspects of production including • Raw or starting materials • Finished products • Premises and environment • Equipment • personnel • Training • Hygiene
GMP Principles • Must be built into manufacturing process • Prevents errors that cannot be eliminated through quality control of finished product • Ensures all units of a medicine are of the same (within specified parameters) quality • Poor medicines leads to loss of credibility for everyone: manufacturers, health care workers and governments • WHO Guidelines for GMP
WHO Technical Guide to GMP • First prepared in 1967 • Updated and revised regularly • “Quality Management in the Drug Industry” outlines general concepts and principle components of GMP • “Good practices in production and quality control” describes implementation
WHO Technical Guide to GMP General Consideration “Licensed pharmaceutical products should be manufactured only by licensed manufacturers whose activities are regularly inspected by competent national authorities”
WHO Technical Guide to GMP Key Concepts • Validation Action of proving (in accordance with principles of GMP) that any procedure, process, equipment, material, activity, or system actually leads to expected results
WHO Technical Guide to GMP Key Concepts • Qualification Action of proving that any premises, system, and items of equipment work correctly and actually lead to expected results
Associated Concepts • Good Laboratory Practice (GLP) • Good Clinical Practice (GCP) • Clear language use • Effective record keeping • Design, installation, operational and process qualification (DQ, IQ, OQ and PQ) • Self-inspection and self-regulation • Good Distribution Practice (GDP)
Key Elements of GMP (WHO Technical Guide) • Sanitation and hygiene • Qualification and validation • Complaints • Product recalls • Contract Production and Analysis • Self-Inspection and Quality Audits
Key Elements of GMP (WHO Technical Guide) Personnel (Training, Hygiene) DocumentationPremises (Equipment) Materials (Supplies, Ingredients)
Product Selection Issues • Unique nature of medicines heightens need for effective quality assurance • All medicines used must be safe, effective, and of consistent quality • Failure to select proper products will lead to treatment failure, drug resistance, wasted resources and human suffering
Product Selection Issues (Cont.) Selection of product and goal of treatment may vary depending upon patient group • Infected adults • Infected women (who may be/may become pregnant) • Infected children (blood-borne or sexual transmission) • Emergency workers • Victims of sexual assault
Demographic Profile of HIV Patients Source: (Zaheer et al., 2003)
Demographic Profile of HIV Patients (Cont.) Source: (Zaheer et al., 2003)
Clinical Outcomes Successful treatment for HIV with quality medicines will: • Improve general health status/well-being • Reduce viral load to <20 cells/mL • Maintain CD4 within normal range (550-1400 cells/mL) • Prevent/reduce drug resistance • Manage and minimize drug-related side-effects • Reduce need for medical intervention
WHO Essential Medicines Categories (for HIV) • NRTIs (Nucleoside reverse-transcriptase inhibitors) (e.g. AZT, ddI, 3TC) • NNRTIs (Non-nucleoside reverse-transcriptase inhibitors) (e.g. NVP, EFV) • PIs (Protease Inhibitors) (e.g. ritonavir, saquinavir) • In the future: Fusion Inhibitors, Integrase Inhibitors
Combination Products • More convenient, improve adherence, reduce pill burden for patient • E.g. Triomune (NRTI-NNRTI triple combination therapy consisting of stavudine, lamivudine, and nevirapine) • Product formulations to allow twice daily (or even once daily) dosing
Use of Medicines in Women Who are Pregnant Acceptable combination treatments d4T + 3TC + NVP ZDV + 3TC + NVP Combination treatments to avoid d4T + 3TC +EFZ ZDV + 3TC + EFZ
Suppliers/Manufacturers “Many reliable manufacturers, both innovator and generic companies, can offer quality products…the aim…is sustained, consistent and acceptable quality rather than high or better quality, terms that are impossible to quantify” Battling HIV/AIDS, World Bank 2004
Sources of Pharmaceutical Products Multi-source Well-established products, long history of use, no longer subject to patent protection (e.g. Rifampin) Single source Newer products still subject to patent protection in many countries (e.g. Saquinavir) Limited source More than single source/supply possible (e.g. AZT); may be difficult to manufacture (e.g. amphotericin); may be unprofitable drug with limited market potential
Identifying Product Suppliers Systematic Approach • Pre-qualification of suppliers and products • Specifying supplier conditions in contract • Monitoring quality of product and processes • Continuous evaluation of supplier performance and product performance in clinical practice
Identifying Product Suppliers Specify Conditions Evaluate Monitor
Selecting and Sourcing Multi-Source Products • Innovator vs. generic issues • Prequalification systems • Specific issues related to interchangeability of products - stability, bioavailability, bioequivalence, etc.
Selecting and Sourcing Multi-Source Products • Innovator vs. generic issues • Prequalification systems • Specific issues related to interchangeability of products - stability, bioavailability, bioequivalence, etc.
Procedures for Prequalification of Suppliers Rationale More meaningful, effective, efficient and less expensive to eliminate sub-standard manufacturers and products at the opening of bidding/tendering than during the process Purpose To ensure that products are manufactured in compliance with GMP and products meet established quality standards
Procedures for Prequalification of Manufacturers • Local Procurement Committee comprising managerial, technical, and professional staff • Manufacturers submit dossiers for review; must be reviewed/re-inspected every 3-5 years to ensure adherence to policies • Review/re-inspection also performed if product changes occur that may impact on safety, efficacy, quality, manufacturing method, or location of manufacturing
Procedures for Prequalification of Manufacturers (Cont.) • Evaluation of Product Dossier • Random testing of samples • Verification of compliance with GMP • Verification of compliance with good distribution practices • Role of national drug regulatory organizations (in compliance with WHO standards)