Download
1 / 47
470 likes | 538 Views
VISN 8 Patient Safety Center of Inquiry: Journey for Change: Innovations to Reducing Fall Incidence and Injury. Thursday, Oct 25, 2012. Pat Quigley, PhD, MPH, ARNP, CRRN, FAAN, FAANP.

E N D
VISN 8 Patient Safety Center of Inquiry: Journey for Change:Innovations to Reducing Fall Incidence and Injury Thursday, Oct 25, 2012
Pat Quigley, PhD, MPH, ARNP, CRRN, FAAN, FAANP Patricia Quigley, PhD, MPH, ARNP, CRRN, FAAN, FAANP, Associate Director, VISN 8 Patient Safety Center of Inquiry, is both a Clinical Nurse Specialist and a Nurse Practitioner in Rehabilitation. As Associate Chief of Nursing for Research, she is also a funded researcher with the Research Center of Excellence: Maximizing Rehabilitation Outcomes, jointly funding by HSR&D and RR&D. Her contributions to patient safety, nursing and rehabilitation are evident at a national level – with emphasis on clinical practice innovations designed to promote elders’ independence and safety. She is nationally known for her program of research in patient safety, particularly in fall prevention. The falls program research agenda continues to drive research efforts across health services and rehabilitation researchers.
Julia Neily, RN., M.S., M.P.H. Julia Neily, RN, MS, MPH, has worked for the VA in various nursing roles for 26 years. She is currently the Associate Director of the NCPS Field Office. She joined the VHA National Center for Patient Safety in 2002 and has focused on fall and fall related injury prevention and evaluation of patient safety efforts such as cognitive aids, Ensuring Correct Surgery and Medical Team Training. Julia has a BS in Nursing from the University of New Hampshire, a Master of Science from New Hampshire College and a Masters of Public Health from Dartmouth Medical School.
Mary Watson, MS, ARNP Mary Watson, MS, ARNP, has been a nurse for 44 years. She received her Master’s in Nursing over 23 years ago and has worked at the VA in Little Rock ever since. Mary is a Gerontological CNS and has worked in the capacity as a Falls Clinical Specialist for 12 years managing her facility’s Fall prevention program and providing Fall consult services to nurses. She has collaborated with Pat Quigley on several projects, including an article published in the Online Journal of Nursing in 2007 entitled “Measuring Fall Program Outcomes.” Mary feels fortunate to be able to lecture locally and nationally on Fall Prevention to help individuals as well as facilities reduce fall-related injuries.
Acknowledgements NCPS VISN 8 Network James A. Haley VAMC IHI Faculty VISN 8 PSCI Partners You!
Program Goal To provide VHA healthcare and quality teams with tools and strategies to reduce preventable falls incidence, injury from falls and outline key components of sustaining and spreading successfully.
Objectives • Inventory tests of change in fall and injury prevention interventions • Differentiate types of falls as a basis for analysis of program effectiveness • Integrate injury prevention into existing fall prevention programs • Summarize successes ready for adoption and spread
Looking Ahead Eight Sessions of Learning and Sharing • Oct 25th: State of Science of Falls and Injury Prevention • Nov 8th: Preventing Falls with Injury Assessment • Nov 29th: Interventions to Reduce Falls and Harm, Part 1 (Equipment and Technology) • Dec 20th : Sustain and Spread Improvements in Reducing Falls and Injury from Falls • Jan 3rd: Injury Risk Assessment and Communication of Risk • Jan 17th: Interventions to Reduce Falls and Harm, Part 2 (Intentional Rounding, Pre-shift Huddle, Post Fall Huddles) • Jan 31st: Use of VANOD, NDNQI and SPOT Databases for Fall Program Evaluation • Feb 7th: Summary of Your Accomplishments
Session Design Welcome and share innovations Work in Teams if Possible Learn and Share Together Suggested assignments at end of each session Questions and answers Engage each other online
Session 1: Readiness for Change • Provide an overview of current body of knowledge about reducing falls and fall injury • Differentiate Types of Falls: Preventable and Unpreventable • Prepare for aim setting and measurement • Present self assessment tools
Successful QI Teams • Produce better outcomes clinically and financially • Know one another’s other’s strength and weaknesses, respect each other, and have often worked together as a team in the past • View their goals to be part of the organization’s key strategic goals • View their team leaders as competent, with the clout to remove barriers to change • Have more time to complete goals and information systems that are helpful to them • Have support from front-line staff • Mills, P. & Weeks, W.B.(2004). Characteristics of successful quality improvement teams: Lessons from five collaborative projects in the VA. Journal on Quality and Safety. 30(3): 152-162
New 2007 JCAHO Standard: Fall Prevention Program • Establish a Fall Prevention Program • Evaluation • Interventions • Educate Staff • Educate Patients and Families • Program Evaluation
Patient Falls and Injuries State of the Science
Prevention • The act of preventing, forestalling, or hindering
Protection • Shield from exposure, injury or destruction (death) • Mitigate or make less severe the exposure, injury or destruction
Review Research, Clinical and Laboratory Information Is evidence strong enough to warrant practice change? Yes Implement evidence- based practice No Does evidence support clinical trials? Technology Transfer Clinical trial to test interventions Yes Equipment design or redesign with evaluation Yes No Is equipment ready for Market? Epidemiological study to identify modifiable risk factors for adverse events or descriptive studies to understand process and outcomes Equipment design or redesign OR
Preventing Falls • Transform healthcare for frailty associated with old age. • Prevent falls identified as an effective strategy. • BUT, major area for improvement in routine practice. • 2003: IOM: Priority areas for national action: transforming health care quality • Multifaceted and individualized fall prevention programs used inside and outside hospital setting. • Thorough review of the strategies revealed they lack strong empirical evidence. • Clyburn, T.A., & Heydemann, J.A. (2011). Fall prevention in the elderly: analysis and comprehensive review of methods used in the hospital and the home. J. of Am. Academy of Orthopedic Surgeons. 19(7): 402-409.
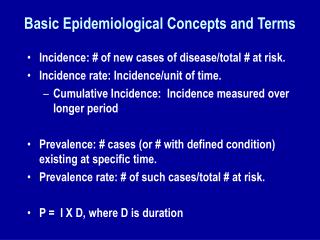
Wu. et al (2010): Epidemiology: Cost Effectiveness of a National Fall Prevention Program • Falls among 65 and older represent major public health and economic burden for US healthcare system • Incidence is high: 1/3 of community dwelling and as many as ¾ of nursing home residents fall each year. • Of those who fall, 20%-30% suffer consequences such as hip fractures/head trauma, reduced mobility and independence, increased risk of early nursing home admission, and premature death • Updated to 2010 dollars, 1 fall without serious injury incurred additional annual cost of about $3500 compared to those with no fall • Those who had 2 or more falls without serious injures, costs increased by about $16,500 • One or more falls involving at last 1 serious injury were costliest: increasing healthcare costs by $27,000. • By 2020, more than 4 mil older Americans projected to incur a fall with injury annually, total cost about $47 bil (adjusted to 2010 dollars)
Conclusion • No conclusive medical evidence that multifactorial prevention programs in the acute hospital settings are effective. • No studies demonstrating statistically significant evidence that any of the individual measures used in the hospital that are often considered to be effective in reducing fall risks are effective, with the exception of addressing delirium • Most current recommendations are based on expert opinion. • Most current recommendations do not increase harm or fall risk, and thus may be safely continued • Outside the hospital, multimodal fall prevention programs that include exercise programs, nutrition, and vision care, along with home evaluations for high risk patients, have been shown to be effective. • Need further investigations, esp. RCTs, in hospitals.
Role of RCTs Parachute use to prevent death and major trauma related to gravitational challenge: systematic review of randomised controlled trials Gordon C S Smith, Jill P Pell. BMJ 2003;327
Etiology, Natural History • A fall usually doesnot have a single cause, but rather, it results from the interaction of a number of intrinsic and environmental factors. • Therefore, the natural history of each fall is different depending on the type of fall: • accidents • anticipated physiological falls • unanticipated physiological falls
Limits to Science • Failure to Differentiate Type of Fall • Accidental • Anticipated Physiological • Unanticipated Physiological (Morse 1997) • Intentional Falls • Which types are preventable and unpreventable? • Failure to Link Assessment with Intervention
Limits to Science • Failure to Differentiate Fall Prevention and Fall Protection • Failure to Examine Risk Factors and Tailor Interventions for Specific Sub Populations • E.g., Wheelchair Fallers
Where are we? Best Practices: Level of Evidence
What is Known: Tried and True The (most effective) fall prevention programs are multifactorial and interdisciplinary (AHRQ I-II, USPSTF A): LTC; Ambulatory Care; Source of Policy for JCAHO Fall Program Guidance 2007
Must Reads: Clinics in Geriatric Medicine, Nov. 2010. Clinical Nursing Research, Feb 2012
Ambulatory Care • AGS, BGS Clinical Practice Guidelines 2010:Prtion of falls in older adults. • Assessment • Interventions • Evidence Grades • Bibliography • www.americangeriatrics.org/health_care_professionals/clinical_practice/clinical_guidelines_recommendations/2010
Interventions AGS Guidelines 2010 Assessment
Hospital Falls: we know…. D. Oliver, et al. Falls and fall-related injuries in hospitals. (2010, Nov). Clinics in Geriatric Medicine. • 30% to 51% of falls result with some injury • 80% - 90% are unwitnessed • 50%-70% occur from bed, bedside chair or transferring between the two; whereas in mental health units, falls occur while walking • Risk Factors: Recent fall, muscle weakness, behavioral disturbance, agitation, confusion, urinary incontinence and frequency; prescription of “culprit drugs”; postural hypotension or syncope
Most effective, fall prevention interventions should be targeted at both point of care and strategic levels • Best Practice Approach in Hospitals: • Implementation of safer environment of care for the whole patient cohort (flooring, lighting, observation, threats to mobilizing, signposting, personal aids and possessions, furniture, footwear • Identification of specific modifiable fall risk factors • Implementation of interventions targeting those risk factors so as to prevent falls • Interventions to reduce risk of injury to those people who do fall (Oliver, et al., 2010, p. 685)
New Tests of Change • New Clinical Practices • New Patient Education Strategies • New Environmental Safety and Technology Innovations
Setting the Stage For Change • Aim Statement • Examine Gap between current performance and stated aim • Learn from falls with serious injuries (try to study 5 or more injurious falls – spirit of discovery)
Aim Setting • What will be done • Within what timeframe • Outcome that is measureable • Short term aim • By the completion of this learning session, we will have achieved 100% compliance with fall risk and injury risk assessment on admission, and the practice of post-fall assessment after each fall event. • Long term aim • By Jan 2013, falls with serious injury will be decreased by at least 30% on 4 West.
Reducing Patient Injury from Falls • Assess Risk of Falling and Risk for a Serious / Major Injury from a Fall • Communicate and Educate (Staff, Patients and Family Members) • Standardize Interventions for Patients at Risk for Falling • Customize Interventions for Patients at Highest Risk of a Fall-Related Injury Our Aim: Achieve a 95% or better reliability for each process step
Complete a baseline Team Assessment:Ask 3 questions: • Compared to This Time Last Year, Now We Are Able To Do . . 2. The Most Important Thing We Learned About Patients at Risk for Harm From Falls Is . . . 3. The Most Important Thing Our Nursing Team Learned About How to Reduce Harm From Falls Is . . .
Reducing Falls vs. Reducing Harm From Falls • Paradigm shift • Assumptions • Promising ideas • Added to current falls prevention programs • Tools for shifting practice emphasis
Self Assessments: Preventing Falls with Injury • VISN 8 PSCI: Organizational Self Assessment Tool • IHI Safety Cross • Minnesota Hospital Association: SAFE from FALLS map
Self Assessment • Let’s review the Organizational Self Assessment Tool
Safety Cross: Adverse Event Incidence Tracking Tool No incidence Incidence Aim: To acquire a green cross or decrease the number of red squares (time between)
Database How do I use this tool? 1. Decide on your safety measures and complete the Setup sheet 2. Print out the Safety Cross for each of your selected safety measures and display for staff to readily see 3. Collect the dates that safety events happen and enter them into the Data Entry sheet 4. View your performance on the Charts sheet
MHA Tool • SAFE from FALLS ROAD MAP
Fall Analysis Tool • Excel Spreadsheet for Analysis of Post Injurious Falls
Session 2 • Integrate Fall Risk Screening, Assessment and Comprehensive Assessment • Apply Clinical Judgment and Expertise to Patient Care and Vulnerable Patients • Utilize the ABCS Framework to segment vulnerable patients, focusing on both fall and injury risk • Examine new patient learning strategies for care transitions.
Assignments for Session 2 • Declare aim statement(s) for fall work including the fall risk assessment tool AND risk for injury tool that you are using or will be utilized • Analyze the gap between current performance and stated aim • Audit last 5 falls with serious injury using Injurious Fall Data Collection Tool • Complete baseline team assessment: Preventing Falls with Injury
Next Session Thursday, Nov 8, 2012 12N-1PM ET