Download
1 / 1
10 likes | 125 Views
NIMH - R01 MH65163-01: Brazilian HIV Prevention for the Severely Mentally Ill - Inside The Institution: Ethnography Demonstrates The Need for an HIV Prevention Intervention

E N D
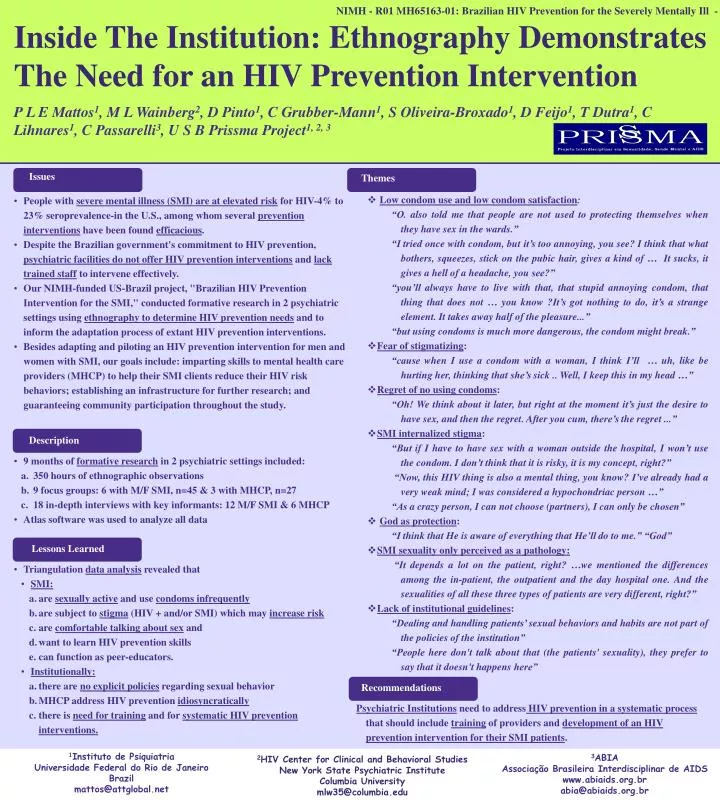
NIMH - R01 MH65163-01: Brazilian HIV Prevention for the Severely Mentally Ill - Inside The Institution: Ethnography Demonstrates The Need for an HIV Prevention Intervention P L E Mattos1, M L Wainberg2, D Pinto1, C Grubber-Mann1, S Oliveira-Broxado1, D Feijo1, T Dutra1, C Lihnares1, C Passarelli3, U S B Prissma Project1, 2, 3 • Issues • People with severe mental illness (SMI) are at elevated risk for HIV-4% to 23% seroprevalence-in the U.S., among whom several prevention interventions have been found efficacious. • Despite the Brazilian government's commitment to HIV prevention, psychiatric facilities do not offer HIV prevention interventions and lack trained staff to intervene effectively. • Our NIMH-funded US-Brazil project, "Brazilian HIV Prevention Intervention for the SMI," conducted formative research in 2 psychiatric settings using ethnography to determine HIV prevention needs and to inform the adaptation process of extant HIV prevention interventions. • Besides adapting and piloting an HIV prevention intervention for men and women with SMI, our goals include: imparting skills to mental health care providers (MHCP) to help their SMI clients reduce their HIV risk behaviors; establishing an infrastructure for further research; and guaranteeing community participation throughout the study. • Description • 9 months of formative research in 2 psychiatric settings included: • 350 hours of ethnographic observations • 9 focus groups: 6 with M/F SMI, n=45 & 3 with MHCP, n=27 • 18 in-depth interviews with key informants: 12 M/F SMI & 6 MHCP • Atlas software was used to analyze all data • Lessons Learned • Triangulation data analysis revealed that • SMI: • are sexually active and use condoms infrequently • are subject to stigma (HIV + and/or SMI) which may increase risk • are comfortable talking about sex and • want to learn HIV prevention skills • can function as peer-educators. • Institutionally: • there are no explicit policies regarding sexual behavior • MHCP address HIV prevention idiosyncratically • there is need for training and for systematic HIV prevention interventions. • Themes • Low condom use and low condom satisfaction: “O. also told me that people are not used to protecting themselves when they have sex in the wards.” “I tried once with condom, but it’s too annoying, you see? I think that what bothers, squeezes, stick on the pubic hair, gives a kind of … It sucks, it gives a hell of a headache, you see?” “you’ll always have to live with that, that stupid annoying condom, that thing that does not … you know?It’s got nothing to do, it’s a strange element. It takes away half of the pleasure...” “but using condoms is much more dangerous, the condom might break.” • Fear of stigmatizing: “cause when I use a condom with a woman, I think I’ll … uh, like be hurting her, thinking that she’s sick .. Well, I keep this in my head …” • Regret of no using condoms: • “Oh! We think about it later, but right at the moment it’s just the desire to have sex, and then the regret. After you cum, there’s the regret ...” • SMI internalized stigma: • “But if I have to have sex with a woman outside the hospital, I won’t use the condom. I don’t think that it is risky, it is my concept, right?” • “Now, this HIV thing is also a mental thing, you know? I’ve already had a very weak mind; I was considered a hypochondriac person …” • “As a crazy person, I can not choose (partners), I can only be chosen” • God as protection: • “I think that He is aware of everything that He’ll do to me.” “God” • SMI sexuality only perceived as a pathology: “It depends a lot on the patient, right? …we mentioned the differences among the in-patient, the outpatient and the day hospital one. And the sexualities of all these three types of patients are very different, right?” • Lack of institutional guidelines: • “Dealing and handling patients’ sexual behaviors and habits are not part of the policies of the institution” • “People here don't talk about that (the patients' sexuality), they prefer to say that it doesn't happens here” • Recommendations • Psychiatric Institutions need to address HIV prevention in a systematic process that should include training of providers and development of an HIV prevention intervention for their SMI patients. 1Instituto de Psiquiatria Universidade Federal do Rio de Janeiro Brazil mattos@attglobal.net 3ABIA Associação Brasileira Interdisciplinar de AIDS www.abiaids.org.br abia@abiaids.org.br 2HIV Center for Clinical and Behavioral Studies New York State Psychiatric Institute Columbia University mlw35@columbia.edu