Download

1 / 48
490 likes | 1.01k Views
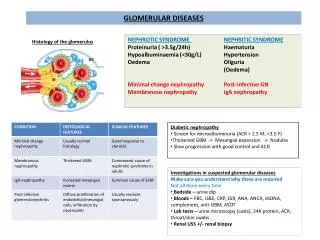
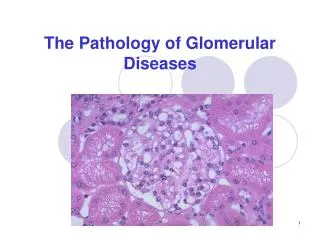
Glomerular Diseases. Dr. Atapour. Differential diagnosis and evaluation of glomerular disease. CLINICAL PATTERNS OF GLOMERULAR DISEASE . Nephrotic Nephritic. Nephrotic pattern . The nephrotic proteinuria that is usually above 3.5 g/day Lipiduria Edema Hyperlipidemia

E N D
GlomerularDiseases Dr. Atapour
CLINICAL PATTERNS OF GLOMERULAR DISEASE • Nephrotic • Nephritic
Nephrotic pattern • The nephroticproteinuria that is usually above 3.5 g/day • Lipiduria • Edema • Hyperlipidemia • Some patients also have microscopic hematuria • Red cell casts
Asymptomatic proteinuria • Full-blown nephrotic syndrome
The bland sediment • Absence of immune complex deposition in most of these disorders: • Minimal change disease • Focal segmental glomerulosclerosis • Diabetic nephropathy • Amyloidosis.
Lack of inflammation • The serum creatinine concentration
Acute kidney injury in the nephrotic syndrome • Concurrent acute tubular necrosis • Usually in minimal change disease
Nephritic pattern • Presence of red cells • White blood cells • Red cell • Dysmorphic appearance • Acanthocytes • Mixed cellular casts • Variable degrees of proteinuria
dysmorphic RBCs muddy brown casts tubular cell casts oval fat body
Pathologic classification • Light microscopy • Focal • Diffuse • This terminology is most often used in lupus nephritis • ANCA-positive vasculitis.
Limitations of this classification • Same pathology and multiple causes • Nonspecific nature of the histologic patterns
MPGN Can be a systemic immune complex disease • To infective endocarditis • Systemic lupus erythematosus • Hepatitis C virus complement
Membranous nephropathy • Systemic lupus erythematosus • Chronic hepatitis B virus infection • Underlying malignancy • Drugs
Focal segmental glomerulosclerosis • Primary condition • Secondary change induced by intraglomerular hypertension or healing of previous glomerular injury.
Nephrotic syndrome without a nephritic sediment • Mild hematuria • No red cell casts
Depend on age What do you think?
Less than 15 years : • Minimal change disease • Focal segmental glomerulosclerosis • Mesangial proliferative glomerulonephritis
15 to 40 years : • Minimal change disease • Membranous nephropathy • Focal segmental glomerulosclerosis • Diabetic nephropathy • Preeclampsia • Postinfectiousglomerulonephritis
Greater than 40 years: • Focal segmental glomerulosclerosis • Membranous nephropathy • Diabetic nephropathy • Minimal change disease • IgA nephropathy • Primary amyloidosis • Benign nephrosclerosis • Postinfectiousglomerulonephritis
Mild glomerulonephritis • Mild glomerulonephritis is defined as a nephritic sediment and: • Normal or near normal estimated GFR • Do not have the nephrotic syndrome
Less than 15 years • Mild postinfectiousglomerulonephritis • IgA nephropathy • Thin basement membrane disease • Hereditary nephritis • Henoch-Schönleinpurpura • Mesangial proliferative glomerulonephritis
15 to 40 years • IgA nephropathy • Thin basement membrane disease • Lupus nephritis, hereditary nephritis • Mesangial proliferative glomerulonephritis
Greater than 40 years • IgA nephropathy
Moderate to severe glomerulonephritis • Moderate to severe glomerulonephritis is defined as a nephritic sediment • Reduced estimated GFR • Nephrotic syndrome ±
Less than 15 years • Postinfectiousglomerulonephritis • Membranoproliferativeglomerulonephritis
15 to 40 years • Postinfectiousglomerulonephritis • lupus nephritis • RPGN (crescenticglomerulonephritis) • IgA nephropathy • Fibrillaryglomerulonephritis • Membranoproliferativeglomerulonephritis
Greater than 40 years : • Rapidly progressive glomerulonephritis • Vasculitis • IgA nephropathy • Fibrillaryglomerulonephritis • Postinfectiousglomerulonephritis
In black patients : • Focal segmental glomerulosclerosis (57 percent) • Membranous nephropathy (24 percent) • Minimal change disease (14 percent) • Membranoproliferativeglomerulonephritis, IgA nephropathy, and immunotactoid nephropathy were each present in 1 to 2 percent.
In white patients: • Membranous nephropathy (36 percent), • Focal segmental glomerulosclerosis (23 percent) • Minimal change disease (20 percent) • IgA nephropathy (8 percent) • Membranoproliferativeglomerulonephritis (6%) • Immunotactoidglomerulopathy (6 percent).
Positive family history • Thin basement membrane nephropathy • Hereditary nephritis (Alport syndrome) • Focal segmental glomerulosclerosis are examples:
LABORATORY TESTING IN PATIENTS WITH SUSPECTED GLOMERULAR DISEASE • serum creatinine • serum albumin • complete blood count • Estimation of protein excretion in patients with proteinuria • serologic testing for disorders that cause glomerular disease • measurement of serum complement levels
membranous nephropathy • The value of hepatitis B virus • Hepatitis C virus (HCV) infection • Congenital and secondary syphilis • HIV infection (FSGS)
Chronic bacterial • Endocarditis • Shunt nephritis • Abscesses • Fungal • Parasitic infections can cause
SUMMARY AND RECOMMENDATIONS • There are many causes of glomerular disease, • the characteristics of the urine sediment, • The degree of proteinuria • Patient’s age often
Two different urinary patterns are seen: • Nephrotic • Nephritic.
The nephrotic pattern = proteinuria > 3.5 g/day • Lipiduria
The nephritic • Red cells • White blood cells • Red cell or mixed cellular casts • Acanthocytes • Some patients have the concurrent presence of two glomerular diseases,
Approaching a patient • Urinalysis • Estimated glomerular filtration rate • Patient age help to identify • Race • Family history • Renal biopsy
Standard laboratory testing • Serum creatinine • Serum albumin • Protein excretion in patients with proteinuria • Serologic testing for disorders that cause glomerular disease
Serologic tests • Lupus • Amyloidosis • Hepatitis B (HBV) • Hepatitis C (HCV) • HIV infection • ANA • Anti-dsDNA • C3 • C4
Primary amyloidosis and light chain deposition disease • Serum and urine immunofixation • Serum free light chain ratio analysis
Glomerulonephritis Nephritic urine RBCs, RBC casts Low – mod proteinuria Nephrotic urine No casts, few RBCs Heavy proteinuria • Diabetes • Amyloid • Membranous Nephropathy • FSGS • Minimal Change Disease • Sometimes MPGN C3, C4 Low Normal • Postinfectious • Lupus nephritis • MPGN (often Hep C) ANCA (+) ANCA (-) • Vasculitis • Wegener’s • MPA • Churg-Strauss • IgA nepropathy • Anti-GBM/Goodpasture’s progress fast progress slow