Download
1 / 68
700 likes | 1.29k Views
MANAGMENT OF VASCULAR MALFORMATIONS. RIADH ABID Imaging Departement Elfarabi Sfax Tunisie . INTRODUCTION. Vast / varied clinical / evolutionary / prognosis : variability Subiquitous : Multiple specialistis Nomenclature and classification. CLASSIFICATIONS.

E N D
MANAGMENT OF VASCULAR MALFORMATIONS RIADH ABID Imaging DepartementElfarabi Sfax Tunisie
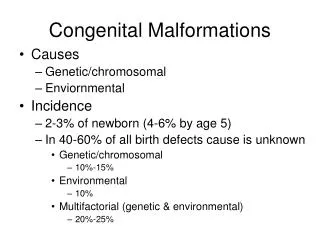
INTRODUCTION • Vast / varied • clinical / evolutionary/ prognosis: variability • Subiquitous: Multiple specialistis • Nomenclature and classification
CLASSIFICATIONS • Merland J.J: Ann.Chir.Plast: 1980, 2, 105. • Muliken J.B : Plast Recons. S: 1982, 69, 412 • Hambourg classification: 1988/1989 • Iternationnal Society for the Study of VascularAnomamlies (ISSVA Rome 1996) • The IAN Jackson classification 1993 • The orbital society classification J Rootman
VASCULAR ANOMALIES VASCULAR TUMOURS ADULT VASCULAR TUMOURS INFANT VASCULAR MALFORMATIONS LOW FLOW Capillary malformations CM Venous malformations VM CMV Lymphatic malformations LM HIGH FLOW Arteriovenousfistula AVF Arteriovenous malformations AVM HEMANGIOMA RCIH NCIH
HEMANGIOMA • transienterror of vascular morphogenesis • proliferation of endothelial cells identical to the parenchyma angioformateur • endothelial marker, GLUT-1: +
HEMANGIOMA / CLINICAL • threeclinical types: Tuberous subcutaneous Mixed
HEMANGIOMA / EVOLUTION Evolution triphasic spontaneouslyresolvent • Is mostly not presentatbirth • Is discoveredafter a few weeks • Growsdisproportionallyuntil 6 or 9 months • Still stable until 18 month • Involuteslowly in 3 or 5 years
HEMANGIOMA / HOW TO BEHAVE • Imaging : not required • mainlyecho Doppler • seldom MRI • How to behave • Abstention in 90% of cases(monotoring) • therapeutic intervention in 10% of cases • Corticotherapy local or general • Avlocardyl • surgeryrepararatrice
CAPILLARY MALFORMATIONPORT- WINE STAIN (PWS) • Capillary dilatation • Macularerythemawhichispresentatbirth and persiststhroughout life • Localized or extended • Clinicaldiagnosis • Mostlyaestheticproblem LASER PULSE DYE IS THE TREATMENT OF CHOICE
PWS INDICATOR OF COMPLEX SYNDROMA • false PWS: management seeavm • PWS cutaneous marker of systematized vascular malformation • Sturge Weber Krabbe • KlippelTrenaunay • Parkes Weber
CVM • gradual expansion of the sector venular immediately post capillary with or without agenesis of draining veins swelling • particular ability to invade without cleavage plane of neighboring structures difficultsurgerybleedingrecurrence
CMV / CLINICAL • Compressible blueswelling • No thrill • Local normal temperature • Outbreakspainful and inflammatory
FUNDAMENTALCHARACTERISTIC change in size depending on the position
CMV / IMAGING • Plain X – ray: phleboliths • Echo- Doppler: venous signal • IRM / TDM: depth extension / bone extension • direct opacification: beforesclerotherapy
CMV / DIRECT OPACIFACATION • diagnostic confirmation • number of compartments • appreciation of the venous return
CVM / THERAPEUTIC MEANS • MedicalTreatment • elasticstockings • Low doses of aspirin seem to minimize phlebothromboses • Surgery : • incompleteresection • bleeding • recurrence • Sclerotherpy • Sclerotherpy + Surgery
VENOUS SCEROSING AGENTS • Sodium tetradecylsulphate 3% et 1% • Alcohol / Asolute Ethanol • Ethibloc • Polidocanol /Asclera and Aethoxysklerolcauses fibrosis inside varicose veins, occluding the lumen of the vessel, and reducing the appearance of the varicosity. • Ethanolamine oleate : Ethamolin a sclerosing agent. It works by creating scar tissue inside a swollen or dilated (wider than normal) vein to prevent bleeding.
SCLEROTHERAPY Sclerotherapy induces an inflammatory reaction that will worsen the symptoms during the week following intervention. Analgesics and anti-inflammatory agents (nonsteroidal anti-inflammatory agents or corticoids) must be given to minimize the symptoms. There should be a time delay of 1–3 months between each sclerotherapy session
MECHANISM OF ACTION • scerosant agent causes irritation and inflammation of bloodvesselwalls that will worsen the symptoms during the week following intervention. • Analgesics and anti-inflammatory agents must be given to minimize the symptoms. • healing of this inflammation leads to fibrosis and sclerosis with collapse of cubicles • There should be a time delay of 2–4 months between each sclerotherapy session
Towneedles techniquelow pressure sclerotherapy K.R.HAMZA CIRSE 2011 ALEX. BERNACLE CIRSE 2011
LYMPHATIC MALFORMATION /LM • Vesiculeswithlymphaticfuidwithout flux • Presentatbirth bat canbecameevidentlater /Never regress • Expandwithinflamation
LYMPHATIC MALFORMATION /LM • Clincal: Cystic , Tissue, Mixed • Diagnosis: clinical / ultrasound • Extension : sometimes TDM / IRM • Tretment: • Surgery: recurrence • sclerotherapy
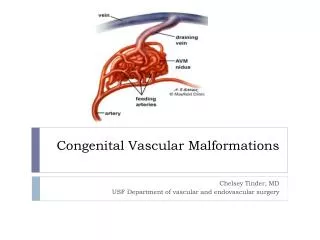
AVM /DEFINITION • Anatomically : abnormal communication without an interposed normal capillary network between artery and a vein • Haemodynamic: • high flow • Active • the most severe vascular malformation and the most difficult to handle Arterycapillaryvein
HIGH FLOW MALFORMATIONS • AVFistulas: a single point of communication betweenfeedingartery and drainingvein • AVMalformations: niduswithseveralarteriel feeders and one severeldrainingveins
AVM / NIDUS It consist of arteriel feeders (alimenteur)and enlargeddrainingveins
AVM / CLINICAL / DIAGNOSIS • Hot mass or swelling red or purplish throbbing with thrill souflante • Bleedingepisodes
AVM / EVOLUTION UNPREDICTABLE • Presentatbirth but maybecameevidentlaiter • Neverr regress • May remain quiescent • Can become evolutionary • Spontaneously • hormonal changes: pregnancypuberty • punctureincompletesurgicalbiopsy
AVM / COMPLICATION Evolutionary AVM Bleeding Ischemianecrosis Cardiacfailure
AVM / /MONITORING • Initial assessment • echo Doppler / • angio CT / MRI • Angiography: subclinical stigma of scalability • Monitoring: regulirement or if Scalability
AVM /CLASSIFICATION / SCHROBINGER • Stage1: lesion-pink-bluish, stain warm, Doppler US- AV shunting (quiescent phase) • Stage 2: lesion –pulsation, thrill, bruit ( expansion phase ) • Stage 3: dystrophic skin changes, bleeding, ulceration, pain (destruction phase) • Stage 4: high output cardiac failure
THERAPEUTIC / MEANS • abstention • Syrgery : • ofteninadequate • Amountbleeding • incompleteresectionwithrecurrence • proximal ligation of the artery should be avoided • ineffective by a develloppement of a network arteriolar • can causes a flare evolutionary • closes the door to the embolization
AVM / THERAPEUTIC MEANS • Embolizationarterialpercutaneousvenous • Combination: arteriel / percutaneous / venous • Multiples sessions
AVM /ANGIO ARCHITECTURE • Uterstanding the anatomy of the various of AV communications is the most important factor to traitingtheseslesions by embolization. • Arterio- venous • Arteriolo-venous • More thanthreefeeding vesselscommunicating • with an identifiable venous sac • Arteriolo-venulous
THERAPEUTIC AGENTS • N-Butylcyano acrylate • Alcohol • Onyx • PVA / Embospheres • Coils • ……
GOALS OF TREATMENT • Control /Prevention of complications / bleeding • Stabilization / control of growth • aesthetic aspects • Curative • Preoperative