Download
1 / 21
210 likes | 417 Views
Managing a swelling in the thyroid. Mark Lansdown Leeds Teaching Hospitals Trust. This presentation will cover -. basic revision difference between diffuse and localised swellings taking a good history

E N D
Managing a swelling in the thyroid Mark Lansdown Leeds Teaching Hospitals Trust
This presentation will cover - • basic revision • difference between diffuse and localised swellings • taking a good history • investigation by the GP (should they be referred immediately or can we usefully scan them) • what you do about them • what GP's need to know about after care of thyroid cancer
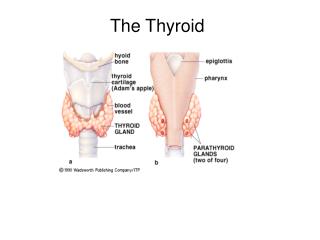
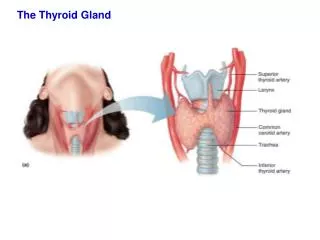
Thyroid - basic revision • first of the body's endocrine glands to develop, at day 24 of gestation • develops from an endodermal thickening in the midline of the floor of the developing pharynx • thyroglossal duct is obliterated, the distal part remaining as the pyramidal lobe • C cells, which produce calcitonin, are of neural crest origin
Thyroid - basic revision 2 • T4 and T3 produced by follicular cells initially as thyroglobulin stored in colloid • Requires iodine (and selenium) • TSH from anterior pituitary regulates production of thyroglobulin and release of T4 into circulation • Active form of thyroxine is T3
Thyroid - basic revision 3 • Thyroxine is essential for normal development and differentiation of probably all tissues of the body • Act on most cells in the adult affecting metabolism, protein synthesis • No pathognomonic symptoms of an under or overactive thyroid
Thyroid - difference between diffuse and localised swellings • Diffuse goitre • Adolescence and pregnancy • Iodine deficiency • Thyroiditis • Early MNG • Localised Swelling (5% population) • Dominant nodule MNG • Cyst • Adenoma • Carcinoma (5% of all nodules)
Thyroid - taking a good history • Symptoms and signs of abnormal thyroid function • T4, TSH, TPO • The “lump” • Since when?, has it changed?, associated symptoms • Pain • Voice change • Medication • Family history
Thyroid - investigation by the GP • T4, TSH • Trends, drifting within the normal range? • Thyroid peroxidase antibodies (TPO) • An anti-thyroid autoantibody • Present in > 90 % Hashimoto’s thyroiditis • Less commonly raised in Grave’s disease, MNG and thyroid cancer
Thyroid - investigation by the GP 2 • Thyroid Ultrasound • Not recommended in the pathway for urgent referrals (2WW) • Highly operator dependent • Often needs to be repeated after referral • Neck ultrasound • incidentalomas
What GP's need to know about after care of thyroid cancer • Is thyroid cancer uncommon? • Incidence USA • Breast 125/100,000 women • Thyroid 20/100,000 women (6/100,000 men) • Prevalence • Breast 3,000,000 • Thyroid 600,000
What GP's need to know about after care of thyroid cancer 2 • THS suppression <0.01 • Not always necessary in the low risk patient • Risk of side effects • Anxiety, palpitations • Bone health • Cardiac health
What GP's need to know about after care of thyroid cancer 3 • Local Guidelines www.ycn.nhs.uk • www.amend.org.uk • www.btf-thyroid.org • www.thca.org (American) • www.butterfly.org.uk