Download
1 / 57
580 likes | 872 Views
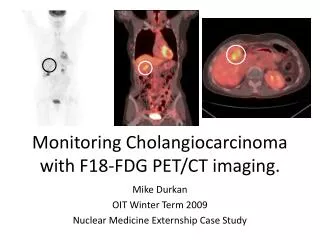
FDG-PET in Indolent Lymphomas. 2009/3/21 新光醫院 核醫科 葉力豪. Case 1. 66 y/o male CC: progressive ptosis with poor visual acuity(os) for 2 years. Cranial CT for orbital study (2007/11/10): suspicious left orbital tumor. Cranial CT for orbital study (2007/11/10). FDG-PET (2007/12/7).

E N D
FDG-PET in Indolent Lymphomas 2009/3/21 新光醫院 核醫科 葉力豪
Case 1 • 66 y/o male • CC: progressive ptosis with poor visual acuity(os) for 2 years. • Cranial CT for orbital study (2007/11/10): suspicious left orbital tumor
FDG-PET (2007/12/7) Orbitl tumor maxSUV:2.8 , Delayed maxSUV:4.5 maxSUV:2.4 maxSUV:2.1 maxSUV:1.7 maxSUV:3.3 maxSUV:3.6 maxSUV:3.9 maxSUV:7.4 maxSUV:1.8
Left Orbital Lesion maxSUV:2.8 Delayed maxSUV:4.5
Left cevical LN 1.0x0.7cm maxSUV:2.4
Pretracheal LN 2.5x1.1 cm maxSUV:3.3 Right axillary LN 1.2x0.8cm maxSUV:1.7
Gastric wall maxSUV:7.4
Gastric wall Delayed image Focal mild FDG uptake maxSUV: 3.4
Right inguinal LN 1.5x0.8cm maxSUV:1.8
Pathology 1. Partial excision of Left Orbital tumor: Marginal zone lymphoma, most likely MALT lymphoma (Extra-nodalMarginal zone lymphoma, Indolent lymphoma) 2. Left inguinal LN biopsy: lymphoid hyperplasia 3. PES with biopsy : ulcer at gastric antrum
Clinical Stage: IIIEBat least Orbital Lesion
Treatment & Follow-up • Chemotherapy as low grade (indolent) lymphoma with Cyclophosphamide : 2008/1/11~4/18 • Partial Remission
Suspcious recurrence since 2008/8/8: A new nodule at left lower eyelid, a LN at suboccipital area Tx with Cyclophosphamide Partial Remission F/U FDG-PET on 2009/1/19
2009/1/19 2007/12/7
Left orbital lesion maxSUV:2.8 lesion subsided
Left cevical LN 1.0x0.7cm maxSUV:2.4 0.9x0.5cm maxSUV:1.9
Pretracheal LN 2.5x1.1 cm maxSUV:3.3 2.3x0.9 cm maxSUV:3.1
Right axillary LN 1.2x0.8cm maxSUV:1.7 0.9x0.5cm maxSUV:1.0
Right inguinal LN 1.5x0.8cm maxSUV:1.8 0.9x0.6cm maxSUV:0.9
Case 2 • 56 y/o male • PH: C-spine and L-spine DJD Gastritis Smoking: (+) , social Drinking: rare • Underwent FDG-PET for physical check-up
2005/12/31 maxSUV:2.4 2007/1/16 maxSUV:3.0
Underwent left lung surgery in NTUH • Pathology: Pulmonary Extra-nodal marginal zone lymphoma (MALT lymphoma)
Marginal zone B-cell lymphoma • The marginal zone lymphomas are so named because of their involvement of the marginal zone surrounding normal lymphoid follicles. • Indolent lymphoma • Three subtypes: 1. Extranodal marginal zone B-cell lymphoma of mucosa-associated lymphoid tissue (MALT) or MALT lymphoma (or Maltoma) 2. Splenic marginal zone B-cell lymphoma 3. Nodal marginal zone B-cell lymphoma
MALT lymphoma • Extranodal marginal zone B-cell lymphoma • May occur in the stomach (most often),orbit, intestine, lung, thyroid, salivary gland, skin, soft tissues, bladder, kidney, and CNS. • May present as a new mass, found on routine imaging studies, or be associated with local symptoms.
MALT lymphoma • Pathology pattern: infiltration of small lymphocyte that are monoclonal B cell and CD5(-). • The majority present with localized stage I or II extranodal disease, involving glandular epithelial tissues of various sites. • In some cases, transformation todiffuse large B cell lymphoma (aggressive lymphoma, worse prognosis) occurs, and both diagnoses may be made in the same biopsy.
MALT lymphoma • These lymphomas can disseminate to other MALT sites, lymph nodes, or marrow in about 30 percent of cases. • In a series of 36 pts presenting with non-GI MALT lymphoma, 12 (33%) were found to have gastric involvement at the time of initial workup. • Some suggest that routine evaluation of the stomach should be a part of the initial staging workup, and at relapse, of non-GI MALT lymphomas Clinical manifestations, pathologic features, and diagnosis of extranodal (MALT) and nodal marginal zone lymphomas. UpToDate
MALT lymphoma • They often arise within tissues involved by chronic inflammatory disorders of autoimmune or infectious etiology: 1. Sjogren syndrome (salivary gland MALT) 2. Helicobacter gastritis (gastric MALT) 3. Chlamydophilapsittaci conjunctivitis (ocular MALT) 4. Borelia skin infection (cutaneous MALT) ★ This neoplasm may lie on a continuum between reactive lymphoid hyperplasia and full-blown B-cell lymphoma.
Treatment of MALT Lymphoma • Localized disease: Local therapy such as radiation or surgery • More extensive disease: Single-agent chemotherapy • Coexistent diffuse large B cell lymphoma: Combination chemotherapy
FDG Uptake Varies Among Different Types of Lymphoma ★ Intensity of FDG uptake determined by: • Histology • Grade • Viable tumor cell fraction • Tumor cell proliferation • Up-regulation of glucose meyabolism • Local perfusion • Presence of hypoxia PET Imaging for Response Assessment in Lymphoma: Potential and Limitation. Radio Clin N Am 46(2008) 225-241
FDG Uptake Varies Among Different Types of Lymphoma • Indolent lymphoma exhibit lower glucosemetabolic activity and hence FDG uptake than the more aggressive ones. • Using an SUV of 10 as a cutoff, FDG-PET seperated aggressive from indolent lymphoma with a sensitivity of 71% and a specificity of 81%. • There is (sometimes large) heterogeneity between lesions of the same histologic entitiy and sometimes overlap between tumor grades. The Impact of Fluorodeoxyglucose-Positron Emmision Tomography in Primary Staging and Patient management in Lymphoma Patients. Radiol Clin N Am 46(2008) 199-211
The Impact of Fluorodeoxyglucose-Positron Emmision Tomography in Primary Staging and Patient management in Lymphoma Patients. Radiol Clin N Am 46(2008) 199-211 FDG Uptake Varies Among Different Types of Lymphoma Aggressive Indolent Indolent Indolent
Diagnostic accuracy of FDG-PET in patients with MALT lymphoma • Overall disease detection sensitivity: In 5 studies (132 pts), 54.4%(18/33) to 81%(21/26, 34/42) • Site dependent: gastric MALT : 38.9%1 & 60%2 non-gastric MALT : 75%1 & 88%2 • Grade dependent: early stage disease (I-II): 42.3%1 & 79%2 advanced disease (stage III-IV): 100% 1,2 • Diagnostic accuracy of PET/CT in patients with extranodal marginal zone MALT lymphoma .Eur J Haematol. 2007 Sep; 79(3):205-9. Epub 2007 Jul 27 • FDG-PET scanning for detection and staging of extranodal marginal zone lymphomas of the MALT type: a report of 42 cases. Annals of Oncology 16: 473–480, 2005
Diagnostic accuracy of FDG-PET in patients with MALT lymphoma • Large cell transformation3: Non-transformed SUV: 3.7 (SD 1.4) Transfromed SUV: 11.3 (SD 5.5) 3. Role of Fluorine-18 Fluoro-Deoxyglucose Positron Emission Tomography Scan in the Evaluation and Follow-Up of Patients With Low-Grade Lymphomas. CANCER July 1, 2006 / Volume 107 / Number 1
Usefulness of FDG-PET in low grade lymphomas Role of Fluorine-18 Fluoro-Deoxyglucose Positron Emission Tomography Scan in the Evaluation and Follow-Up of Patients With Low-Grade Lymphomas. CANCER July 1, 2006 / Volume 107 / Number 1
Large cell transformation (LCT) • Some of indolent lymphomas (about 3% per year) will undergo large cell transformation (histologic transformation) during the course of the disease, an event that dictates a different management strategy and alters survival signicantly. • Although LCT can be suspected on clinical grounds alone, it may also go unnoticed or may be difficult to prove. Role of Fluorine-18 Fluoro-Deoxyglucose Positron Emission Tomography Scan in the Evaluation and Follow-Up of Patients With Low-Grade Lymphomas. CANCER July 1, 2006 / Volume 107 / Number 1
Large cell transformation (LCT) • Significant difference between FDG uptake of nontransformed and transformed lymphomas. • When during the course of an otherwise indolent disease, there are FDG avid foci with much higher uptake than noted on the baseline study, suspicion should be raised regarding LCT. Role of Fluorine-18 Fluoro-Deoxyglucose Positron Emission Tomography Scan in the Evaluation and Follow-Up of Patients With Low-Grade Lymphomas. CANCER July 1, 2006 / Volume 107 / Number 1