Download
1 / 28
290 likes | 785 Views
Early discoveries of brain function and localisation. Dr. Paul Dockree, History of Psychology: PS1203, 2009. What is neuropsychology?.

E N D
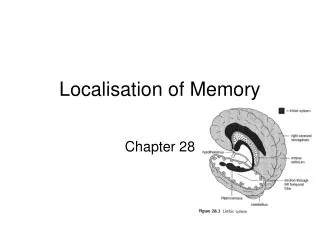
Early discoveries of brain function and localisation Dr. Paul Dockree, History of Psychology: PS1203, 2009
What is neuropsychology? “In any well-made machine one is ignorant of most of the parts – the better they work the less we are conscious of them…it is only fault that draws attention to the existence of a mechanism at all.” (Craik, K., 1943) TV set analogy: Faulty TV sets:- -no sound but intact picture -no picture but intact sound -picture without colour (ie black & white pic) -colour without picture?
What is neuropsychology? • The experimental neuropsychologist asks, “What pattern of behavioural dysfunction occurs when a particular brain region is damaged or lesioned?” • The clinical neuropsychologist asks, “How can normal function be restored or compensated for in the brain?” • Science-Practitioner Model
How did the field evolve? • John Hughlings Jackson’s (1835-1911) first credible human localisationist view – evidence from epileptic patients.
How did the field evolve? Broca’s Aphasia In 1862, showing brain lesions in a stroke patient who could understand language but could not speak (could only say "tan"), he demonstrated that the left frontal lobe was responsible for articulation of speech.
How did the field evolve? Wernicke’s Aphasia Like Broca, Wernicke investigated a similar stroke victim. But this time the patient could speak but made no sense. The damaged area was around where the temporal and parietal lobes meet in the posterior part of the left hemisphere. His findings further revived the localisationist view. Wernicke’s aphasics show deficits in language comprehension but intact articulation
To mean: "The dog needs to go out so I will take him for a walk.“ a Wernicke’s aphasic patient says: “You know that smoodle pinkered and that I want to get him round and take care of him like you want before.” an Broca’s aphasic patient says: “Walk dog.” How did the field evolve? Speech content of a Broca’s and Wernicke’s aphasic
Brain function Structures to be Lesioned Area A Broca’s area Area B Wernicke’s area Function X Speech articulation Impairment Can’t speak fluently No Impairment In fluent speech Function Y Speech comprehension No Impairment Understanding speech of others Impairment Can’t understanding speech of others The logic of lesion analysis Function X: speech articulation Function Y: speech comprehension Area A: Broca’s area Area B: Wernicke’s area
Brain function Structures to be Lesioned Area A Broca’s area Area B Wernicke’s area Function X Speech articulation Impairment Can’t speak fluently No Impairment In fluent speech Function Y Speech comprehension No Impairment Understanding speech of others Impairment Can’t understanding speech of others The logic of lesion analysis Function X: speech articulation Function Y: speech comprehension Area A: Broca’s area Area B: Wernicke’s area
The logic of lesion analysis • Function X (articulation of speech) depends on area A (Broca’s area) but not area B, • whereas function Y (comprehending speech) depends on area B (Wernicke’s area) but not area A. • Double dissociation – Gold standard of neuropsychological research
How did the field evolve? Wilder Penfield • Growing evidence for localisationist view in early 20th century – direct evidence from motor and sensory maps in the brain from early work of Wilder Penfield. • Features drawn according to how much brain space they take up in somatosensory cortex.
How did the field evolve? Wilder Penfield Stimulating the temporal lobes could he elicit meaningful, integrated responses. Physical basis for memory: an "engram.”
How did the field evolve? • Holistic approach: • Karl Lashley (1935) – lesions made throughout the brain do not necessary create problems when learning a new task (e.g., maze learning in rats). • A lesioned brain is like a new system, not an old system with one part missing.
How did the field evolve? • Localisation vs holistic: A Compromise- • Complex functions (e.g., perception, memory, reasoning) cannot be accomplished by a single brain process or brain region; integration of functional neuroanatomy – holistic view • Nevertheless, the simple processes themselves that are recruited to exercise complex functions are localised – localisation view • Brain damage may reveal something about the underlying organisation of the system.
What are the methods used in neuropsychology? • Psychometric testing: • database of standardised scores • Clinical patients vs. healthy controls • Clinical observation: • Diagnosis • Assessment • Rehabilitation • Neuroanatomy: • Connectional studies in animal studies • projection maps (e.g., LGN to visual cortex)
What are the methods used in neuropsychology? • Lesion analysis: • selection of animals or humans with discrete brain damage to areas thought to be essential in a particular processing chain. • one of the oldest methods for studying brain function in humans and animals. • single most informative technique available for understanding the neural bases of behaviour. • http://www.wwnorton.com/college/psych/psychsci2/content/activities/ch04a.asp#movie
What are the methods used in neuropsychology? • Types of lesions: • cerebrovascular accidents (CVA; stroke); occurs when blood flow to the brain is disrupted;
What are the methods used in neuropsychology? • Types of lesions: • penetrating head injuries, from gunshot or other incidents;
What are the methods used in neuropsychology? • Types of lesions: • Following traumatic brain injury (TBI), diffuse white matter damage typically co-occurs with more focal lesions or hematomas (blood clots) and contusions (bruising) damaging the dense collections of cell bodies (grey matter)
What are the methods used in neuropsychology? • Types of lesions: Neurodegeneration: widespread area of tissue death or abnormal cell functioning due to neuropathology (AD, PD); healthy older person Pt with AD
What are the methods used in neuropsychology? • Deliberate lesions - on experimental animals. • tissue excision, where tissue is deliberately removed (usually by aspiration); • tissue destruction, tissue is destroyed electrolytically or chemically (e.g., MPTP, a chemical agent to create an animal model of Parkinson’s disease);
What are the methods used in neuropsychology? • tissue deactivation, where tissue is reversibly deactivated via injections of local anaesthetic or through chemical cooling; • tissue disconnection, where brain areas are left intact but fibre tracts which communicate between these areas are permanently cut or temporarily interrupted (by anaesthetic or cooling);
What are the methods used in neuropsychology? • Neurosurgery is often conducted on humans in order to relieve conditions such as drug-resistant epilepsy (patient H.M.), relief from intractable pain or brain tumours.
Laterality The Wada test: sodium amytal technique • Sodium amytalis injected into one hemisphere at a time • The effect is to shut down any language and/or memory function in that hemisphere in order to evaluate the other hemisphere ("half of the brain"). • Then the patient is engaged in a series of language and memory related tests
Neurorehabilitation • Broca and aphasia therapy (1865) • Broca concluded that the patient, “could recognize a word as one would a face or landscape, the details of which had never been analysed” • it deosn't mttaer waht oredr the ltteers in a wrod are, the olny iprmoetnt tihng is taht the frist and lsat ltteres are at the rghit pclae. The rset can be a tatol mses and you can sitll raed it wouthit a porbelm. Tihs is bcuseae we do not raed ervey lteter by it slef but the wrod as a wlohe.
Neurorehabilitation • WW1- German rehabilitation (Popplereuter, Goldstein) • Cologne and Frankfurt centres • WWII – Alexandra Luria: theoretical perspective from which to predict recovery • Restoration of function via: • De-inhibition • Transfer to opposite hemisphere • Reorganisation of the system • Luria stressed the importance of premorbid personality and motivation
A reading of the last fifteen years of the functional imaging literature - imaging literature largely concerned with the high-tech confirmation of the preceding one hundred and fifty years of careful neuropsychological analysis. PET and fMRI studies do not provide a definitive conclusion about whether or not a particular area is absolutely required in a processing chain. The only way to definitively decide if function X is dependent on area A is to remove that area from the processing chain. Is there any point to lesion analyses now?
Is there any point to lesion analyses now? • Lesion analysis complements functional imaging by identifying necessary and contributing components of the processing chain; functional imaging also allows the identification of specific components of the processing chain. • Overall one strategy complements and underlines the other. • nb:All of the above techniques require that you get the psychology right - if you do not have a good functional theory, applying technology will not get you a meaningful answer. • Further understanding of lesions and their functional role is key for targeted rehabilitation of function and the guided recovery of patients.