Download

1 / 41
430 likes | 1.04k Views
ANGINA PECTORIS. Tb. Tuberculosis. Carl Matol, RN. ANGINA- to choke. CLASSIC/STABLE ANGINA Due to insufficiency of O2 supply against myocardial demand Accumulated effect of sedentary lifestyle and physical inactivity Easily triggered by emotional and physical stress

E N D
ANGINA PECTORIS Tb Tuberculosis Carl Matol, RN
ANGINA-to choke • CLASSIC/STABLE ANGINA • Due to insufficiency of O2 supply against myocardial demand • Accumulated effect of sedentary lifestyle and physical inactivity • Easily triggered by emotional and physical stress • A.K.A. EXERTIONAL ANGINA
VARIANT/RRINZMETAL ANGINA • occurs during rest or with minimal exertion • It is Nocturnal • It follows a cyclic pattern • Dysrrhythmias are present during severe attacks • vasospasm due to hyperactive SNS • A.K.A. VASOSPASTIC ANGINA
UNSTABLE ANGINA • Increase in probability of progressing to MI • Occurs due to sublte/minor injury to atheromatous plaque • A.K.A. PREINFACTION ANGINA No increase in oxygen demand is placed on the Heart muscle, but an acute lack of blood flow to the muscle occurs. 1. Change in frequency, duration, and intensity of stable angina. 2. Last longer than 10 minutes
SILENT ISCHEMIA The ABSENCE of Chest Pain. : Documented by evidence of an imbalance between myocardial oxygen and demand. : Determined by ECG, Exercise Stress Test, or ambulatory [Holter] ECG Monitoring. 1. Occurs in early morning hours [6 AM – 12 PM] 2. Arousal causes increase in sympathetic stimulation and blood viscosity, and coronary vessel tone increase in the morning.
PHARMACOLOGICAL MANAGEMENT • Nitroglycerin (GycerolTrinitrate) • Vasodilating agent (both veins and artery) • Sublingual, Ointment, patch • Beta Blockers • Calcium Channel blockers
Antiplatelets/anticoagulants • ASPIRIN • 160-325 mg dose given to angina pt at ER • 81-325 mg as mainenance medication • ASPIRIN+H2 BLOCS • HEPARIN • A bolus dose may be given and then an IV infusion Q4-6 hours • Watch out for bleeding tendencies
Myocardial Infarction Tb Carl Matol, RN
Nursing Care Management 104: CRITICAL CARE NURSING Disorders of the CARDIOVASCULAR SYSTEM: Myocardial Infarction RISK FACTORS PATHOPHYSIOLOGY : CORONARY ARTERY DISEASE [Atherosclerosis] CORONARY ARTERY SPASM CORONARY ARTERY EMBOLISM Infectious Diseases Arterial Inflammation HYPOXIA ANEMIA Severe Exertion or Stress on the Heart with CAD MYOCARDIAL INFARCTION Untreated: Treated: Drug Therapy: Complications: Thrombolytic Agents Degrees of Damage Occur to the Heart Muscle According to Layers of the Heart Muscle According to Location of Damage within Ventricles Rhythm Disturbances Anticoagulants CARDIAC Failure: Infract Expansion Infract Extension CHF Cardiogenic Shock Reinfarction Zone of Necrosis Transmural [Q Wave] Infarction Left Ventricle Beta-blocking agents Zone of Injury Antidysrhythmic Subendocardial [Nontransmural/Non-Q] Infarction Cardiac Tamponade Calcium Channel Blockers Zone of Ischemia Right Ventricle Pericarditis [2-3 days after MI] Medical Management: Psychiatric Problems: Depression Personality changes Percutaneous Transluminal Angioplasty D E A T H Mortality Bypass Surgery
Nursing Care Management 104: CRITICAL CARE NURSING Disorders of the CARDIOVASCULAR SYSTEM: Myocardial Infarction NURSING MANAGEMENT Nursing Diagnoses: • Pain related to an imbalance oxygen supply and demand • Decreased Cardiac Output related to impaired contractility • Activity Intolerance related to insufficient oxygenation to perform activities of daily living [ADL] • Risk for Injury [bleeding] related to dissolution of protective clots. • Altered Tissue Perfusion [myocardial] related to coronary restenosis, extension of infarction • Anxiety related to chest pain, fear of death, threatening environment
PERCUTANEOUS CORONARY INTERVENTION (PCI) • PTCA • CORONARY ARTERY STENT • ATHERECTOMY
SURGICAL MANAGEMENT • CABG candidates for CABG: • Uncontrolled angina • A positive exercise tolerance test • A blockage of more than 20% on the left main coronary artery • Blockage of two or more coronary artery • Complications from unsuccessful PCI • Left ventricular dysfunction with blockage
Important consideration!!! • For a patient to be considered for CABG, the coronary artery to be bypassed must have at least 70% occlusion • (60% if it is the left main coronary artery)
THE SULTAN REVIEW GROUP NURSING REVIEW CORONARY ARTERY DISEASE: Surgical Management PERCUTANEOUS TRANSLUMINAL CORONARY ANGIOPLASTY [PTCA]
THE SULTAN REVIEW GROUP NURSING REVIEW CORONARY ARTERY DISEASE: Surgical Management CORONARY ARTERY BYPASS GRAFTING (CABG)
NURSING MANAGEMENT: • Promote oxygenation & tissue perfusion – O2 therapy 24-48H or longer, position on semi-fowler’s, avoid overfatigue • Promote adequate cardiac output – monitor ECG, VS, effects of daily activities, give medications • Promote comfort – relieve pain • Provide rest – CBR w/BRP 24-48H, administer diazepam, psychosocial support • Promote activity – gradual increase in activity after 24-48H • Promote nutrition & elimination-small, frequent feedings, low chole, low Na diet, avoid stimulants, avoid very hot or cold beverages.
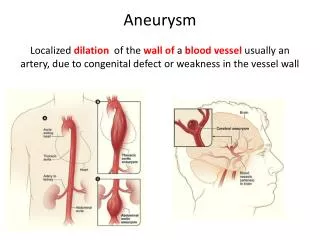
COMPLICATIONS OF MI: • Dysrhythmias • Cardiogenic shock • Thromboembolism • Pericarditis • Rupture of Myocardium • Ventricular aneurysm • CHF