Download
1 / 55
550 likes | 810 Views
University of Uppsala, Sweden. Akuta koronara syndrom på IVA B. Lindahl. Acute Coronary Syndromes. Unstable angina. nonST-elev. MI. ST-elevation MI. Evidence of ischemia – symptoms / ECG changes. Evidence of necrosis – biochemical markers. ST-segment elevation. Stabil kärlkramp.

E N D
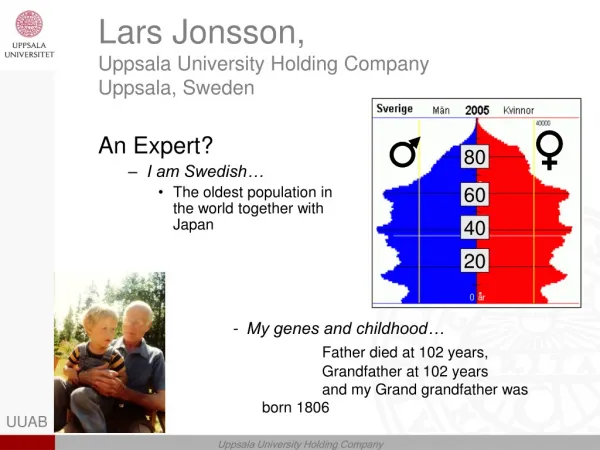
University of Uppsala, Sweden Akuta koronara syndrom på IVA B. Lindahl
Acute Coronary Syndromes Unstable angina nonST-elev. MI ST-elevation MI Evidence of ischemia – symptoms / ECG changes Evidence of necrosis – biochemical markers ST-segment elevation
Stabil kärlkramp Akuta Koronära Syndrom Instabil kärlkramp "vilo-angina" Instabil kärlkramp "acc. angina" ST--infarkt plaque ruptur blodpropps bildning Icke-ST--infarkt Symtomfrihet
5% Mortalitet vid akut hjärtinfarkt hos patienter 65 – 75 år insjuknade 1995-2001
Diagnos • avspegla patogenes • vägleda behandling • prognostisk information
Definition of Myocardial Infarction: Myocardial cell death due to prolonged ischemia ESC/ACC consensus document
Aspects of MI by different techniques Pathology Myocardial cell death Biochemistry Markers of myocardial cell death recovered from blood samples ECG Evidence of myocardial ischemia (ST-T segment changes) Evidence of loss of electrically functioning cardiac tissue (Q-waves) Imaging Reduction or loss of tissue perfusion Cardiac wall motion abnormalities ESC/ACC consensus document
New international (ESC/ACC) criteria for acute, evolving or recent MI • Elevated marker of myocardial damage, preferably troponin T or I, together with at least one of the following: • ischemic symptoms (eg. typical chest pain) • development of pathological Q-waves • ECG changes indicative of ischemia, i.e. ST-segment elevation or depression • coronary artery intervention • Pathologic findings of an acute MI
New international (ESC/ACC) criteria for AMI - additional qualifiers • size – microscopic focal necrosis / small <10 / medium 10-30 / large >30 % of LV • location –ant / lat / inf / post / septal • timing – acute<6/healing6-28/healed>28days • circumstance – spontaneous/procedure related
EKG ST-höjning ( 2 mm i V1-3, 1 mm i övriga avledningar) ST-sänkning ( 0,5 mm) T-vågsnegativitet ( 1 mm) Ca 50 % har ”icke-diagnostiskt” ekg 5-10 % av alla infarkter har normalt ekg vid ankomst Ekg-förändringar är dynamiska
Reciproka ST-sänkningar i anterioseptala avledn. pga ocklusion i vänster koronarartärs cirkumflexa-gren
Egenskaper hos en bra myokardskademarkör • Omätbara nivåer i plasma hos hjärtfriska • Hög koncentration i myokardceller • Exklusivt lokaliserad i myokardceller • Frigörs av irreversibel myokardskada • Lämpligt tidsfönster • Tillgång till snabb och tillförlitlig test
kontraktila enheter troponin T troponin I myoglobin creatine kinase (MM & MB) cellkärna troponin T troponin I Hjärtmuskelcell
Troponin I • funktion reglerande protein i den kontraktila apparaten (inhibitory) • cellokalisation strukturellt bundet 96% - cytosol 4 % • isoformer hjärtmuskel och skelettmuskel • molekylvikt 22,5 kD • analysmetoder: masskonc. (immuno-assay)
Troponin T • funktion reglerande protein i den kontraktila apparaten (binder till tropomyosin) • cellokalisation strukturellt bundet 94% - cytosol 6 % • isoformer hjärtmuskel och skelettmuskel • molekylvikt 37kD (39) • analysmetoder: masskonc. (immuno-assay)
Kreatinkinas (CK) • funktion kreatinfosfat + ADP kreatin + ATP • cellokalisation cytosol • isoenzym CKMB CKMM CKBB • vävnadsdistribution hjärtmuskel 10-20% 80-90% - skelettmuskel 2% 98% - hjärna (tarm) - - 100% • molekylvikt 86 kD 86 kD 86kD • analysmetoder enzymaktivitet eller masskonc. (immunoassay)
False positives/negatives (eg. troponin) • Fibrin • Heterophile antibodies (eg RA) • Human anti-mouse antibodies
Konc URL Tid Tidsfönster Markör initial maximal normalisering CK 4-8 12-24 3-4 d CK-MB 3-6(8) 12-20 48-72 h myoglobin 1-4 6-12 18-36 h troponin T 3-9 12h-4d 6-14 d troponin I 3-9 10-20 4-8 d
Provtagningsschema UAS 0 3 9 24 h • ST-höjning troponin I x x x • Ej ST-höjning troponin I x x x (x) myoglobin endast vid behov (LBBB)
Severity of myocardial damage A M I A M I A M I M M D No A M I New Old Classification CK troponin CK-MB ECG (Q-wave) Diskriminators
10 22 36 57 69 81 100 % CK-MB 20 x URL No evidence of myocardial damage 10 x URL 5 x URL WHO AMI diagnosis (CKMB 2 x URL) 1st gen. troponin I (AxSym 1.0 g/L) 2nd gen. troponin I (Access 0.03 g/L) FRISC-II Non-STelevation ACS
Event rate at one year % 20 18 16 14 12 MI GUSTO-IV at 30-days 10 8 6 4 Death 2 0 TnT <0.01 0.01-0.17 0.18-0.63 >0.63g/L FRISC-II Lindahl et al. JACC oct 2001
Coronary artery disease • increased prevalence of significant stenoses • more complex lesions • increased prevalence of intracoronary thrombi • impaired coronary flow rate and tissue level perfusion • Myocardial necrosis • potential origin of ventricular arrhytmias • at higher levels of troponin (= greater size) cause of reduced left ventricular function • Summary of suggested mechanisms behind the prognostic value of troponins in ACS
Myokardskada Ischemi Andra orsaker till myokardskada (t.ex. myokardit, trauma, cyto- statika etc.) Hjärtinfarkt Förhöjda nivåer av troponin visar att en myokardskada har inträffat, men säger i sig inget om orsaken till denna skada.
Possible causes of elevations of cardiac troponins Primary ischemic cardiac injury · Thrombotic/embolic coronary occlusion (STEMI / non-STEMI) Secondary ischemic cardiac injury · Coronary intervention (PCI / CABG) · Sympathomimetics (cocaine, catecholamine storm) · Pulmonary embolus (presumed right heart strain or hypoxia) · Coronary artery spasm · Coronary artery inflammation (va sculitis) · Prolonged tachyarrhythmia · Acute heart failure · Extreme endurance exercise Non-ischemic cardiac injury · Myocarditis (infection, auto-immune, drugs) · Cardiac trauma · Metabolic/toxic (renal failure, septic shock, drugs)
Hur ofta är troponin (T/I) förhöjt hos ”IVA-patienter”? • Kritiskt sjuka patienter • 9 studier (n=21-260) • Sepsis, pneumoni, COPD, resp-insuff, lungembolism, G-I blödning, post-op etc • Prevalens pos troponin 15-62 %, medel ca 25-30 % • Icke-hjärtkirurgi • 8 studier (n=28-772) • Kärl (inkl aorta), spinal, G-I, ortopedisk, ”general”, thorax (ej hjärt). • Prevalens pos troponin 0-27 %, medel 13%
Kritiskt sjuka patienter – mortalitet (%) i relation till troponinnivå n prev. tn-neg tn-pos Guest et al. 209 15 15 41 p<0.001 Kolleff et al 260 16 16 27 p=0.10 Turner et al 21 62 0 44 ns Ver Elst et al 46 50 30 61 ns Giannitsis et al 56 32 2.6 44 sign Spies et al 26 69 38 83 p=0.02
209 pat Guest et al. JAMA 1995;273:1945-9 ”Medical and respiratory ICU” tn-neg 177 pat tn-pos 32 pat Clinical AMI 12 pat No clinical AMI 20 pat Mortality 15% 42% 40%
ver Elst et al. Clin Chem 2000;46:650-7 ”septic shock” No signs of ischemia during 48 h of ECG-ischemia monioring 46 pat tn-neg 23 pat tn-pos 23 pat LV-dysfunction 9% 78% (p<0.001)
58 pat Ammann et al. J Am Coll Cardiol 2003;41:2004-9 Consecutive critically ill patients admitted for non cardiac reasons (mostly sepsis) tn-neg 26 pat tn-pos 32 pat (55 %) 30 day mortality 5,2 % 22,4 % (p<0.018) LVEF 60 ±10% 48 ±13% (p=0.0006) no significant CAD (stress-echo or autopsy) 72% TNF-alpha (pg/ml) 5.7 13.0 (p=0.0007) Il-6 (pg/ml) 29 358 (p=0.0007)
Troponin and severe hypotensionArlati S et al. Intensive Care Med. 2000;26:31-37 • 31 critically ill patients • reasons for hypotension - septic and hypovolemic shock • mild hypotension syst BP <90 for 30-60 min (HR>100) • severe hypotension syst BP <90 for >60 min (HR>100) no hypot. mild hypot. sev hypot. cTnI (ng/ml) 0.5 1.16 8.50 *
With AMI diagnosis 13.6 % Without AMI diagnosis 33.9 % * TnI in a surgical ICU (I)(retrosp. study) Rene et al. Crit Care Med 2003; 31: 2598-2603)
Peri/post-operativa hjärtinfarkter • Inte alltid trombosorsakad – bt-fall, blödning • Bröstsmärtan ofta ”maskerad” • Omotiverad tachycardi / hypotension • Debut av dyspne / hjärtsvikt • EKG och provtagning (troponin T/I) på vida indikationer
Lopez-Jimenez et al. JACC 1997;29:1241-5 ”noncardiac surgery” Patients with no major cardiac event during index-hospitalisation 6-months follow-up regarding cardiac events (death,AMI, hospitalisation for UA) 772 pat 772 pat tn-neg 680 pat tn-pos 92 pat CKMB-neg 561 pat CKMB-pos 211 pat CE 1.6 % 8.7 % 2.8 % 2.3 % p=0.001 p=0.67
Slutsatser • Troponin stegring talar starkt för någon form av myokardskada/påverkan • Troponin stegring akut hjärtinfarkt • För diagnosen akut hjärtinfarkt krävs troponin stegring + andra tecken talande för hjärtischemi (främst ekg tecken) • Troponin stegring indikerar en sämre prognos även på IVA-patienter
ANP = atrial NP Mainly found in atrium. Pool in granula in cardio-myocytes. Released to blood by hemo-dynamic volume increase ( myocardial stretch ). BNP= Brain NP(originally found in brain) Mainly found in ventricles. Fast synthesis and release to blood by myocardial stretch Natriuretic peptides • Cardiovascular effects of NPs • Syst & pulm vasc resistance; and syst & pulm art pressure • Right atrial & LVEDP • RBF, GFR & urine output Venodilation and coronary artery dilation
NT-proBNP: Synthesis and secretion proBNP(108 amino acids) signal peptide(26 amino acids) BNP 32(physiologically active form) NT-proBNP(1 - 76) R I D S M S K S R S C 1 10 70 76 G F H L C H2N— C —COOH P L G S P G S A S Y T L R A P R C G K S V G L Q V R M R K —COOH H 60-120 min 20 min P H2N— S pre-proBNP(134 amino acids) Cardio-myocyte blood Half-life
Accepted and possible roles for BNP/NT-proBNP in heart disease • Screening and diagnosis of CHF • Risk stratification in CHF • BNP-guided theraphy of CHF • Early risk stratification in ACS • Diagnosis of heart transplantation rejection • Prognosis in pulmonary embolism • Detection of diastolic dysfunction etc…
6. BNP – in acute CHF • 91 patients admitted with acute CHF • mean LV-EF 35 % • BNP and ANP measured after stabilisation of the patient Cox regression analysis on 1-year mortality univariate p-value multivariate p-value Age 0.0007 0.003 Sex NS NS NYHA class 0.02 NS End diastolic dimension NS NS LV-EF 0.001 NS ANP 0.0005 NS BNP <0.0001 <0.0001 Cheuk et al. E J of heart failure 1999;1:59-65)
30 290 ng/L 97.5:th percentile in healthy controls 25 20 15 10 5 40 26 55 106 22 72 185 30 3 16 0 293 2399 <98 184 452 669 1006 1429 >4634 ng / L 1-year mortality in relation to NT-proBNP level James et al. Circulation 2003;108:275-81
2-y mortality P=0.02 % 20 11 / 60 15 NT-proBNP P<0.001 1st-2nd tertile 10 19 / 231 3rd tertile 5 13 / 508 1 / 40 0 LVEF>0.45 LVEF<0.45 Non-invasive group
BNP/NT-proBNP in ICU-patients (I) BNP for detection of significant cardiac dysfunction (cut-off 144 pg/ml) sens 92% spec 86% NPV 96% McLean AS et al. Anaesth Intensive Care. 2003;31:21-7
BNP/NT-proBNP in ICU-patients (II) BNP for detection of cardiac abnormality BNP (pg/ml) 86 without cardiac abnormality 60 98 35 with cardiac abnormality 518 394 Adjusted OR of elevated BNP (cut-off 144 pg/ml) for cardiac abnormality 232 (22-2479) McLean AS et al. Critical Care Med. 2003;31:2611-18
Akut behandling av ACS • Smärtlindring • Anti-ischemisk behandling • Trombosbehandling • Sviktbehandling • Arytmiövervakning/behandling
Anti-ischemisk behandling • Beta-blockad symtomlindring, minskar infarktstorlek, arytmibenägenhet, mortalitet, reinfarktrisk • Nitrater symtomlindring • (Ca-hämmare) symtomlindring diltiazem minskar död/reinfarktrisk
ST-höjninginfarkt • Omedelbar propplösande behandling • trombolys / akut PTCA
Nytta av propplösande behandling – de gyllene första två timmarna