Download
1 / 78
870 likes | 2.66k Views
Fractures of the Femur, Tibia, and Fibula. Presented by: Dr. Aric Storck October 2, 2002. Objectives. Clinical evaluation Radiological diagnosis Emergency department management Will not discuss hip fractures (femoral head, neck, trochanters) – discussed at pelvis/hip rounds

E N D
Fractures of the Femur, Tibia, and Fibula Presented by: Dr. Aric Storck October 2, 2002
Objectives • Clinical evaluation • Radiological diagnosis • Emergency department management • Will not discuss hip fractures (femoral head, neck, trochanters) – discussed at pelvis/hip rounds • Will not discuss distal tib/fib fractures -discussed during ankle rounds
Femur FracturesFemoral Shaft Fractures • High-energy trauma – MVC, bicycle, falls • Tensile strain usually produced transverse fractures • Comminution with higher forces • Open fractures uncommon – generally penetrating trauma • Pathologic fractures – result from torsional stress causing spiral fracture
Femoral Shaft FractureClassification • No generally accepted system • Describe based on characteristics • Location • Geometry • Transverse, oblique, spiral, wedge, comminution
Femoral Shaft FracturesClinical Features • Obvious deformity • 50% have ligamentous instability of the knee • Neurovascular injuries rare in closed fractures • Fracture of Proximal 2/3 • Proximal fragment abducted, flexed, and externally rotated due to pull of gluteal and iliopsoas muscles of trochanters • Fracture of Distal 1/3 • Hyperextension of distal fragment due to pull of gastrocnemius
Femoral Shaft FracturesED Management • Cross and type for at least 2 units PRBC • Assess and treat neurovascular status • D/C traction (NV damage more likely from traction than from fracture) • Immobilize without traction • Analgesia (im/iv or femoral nerve block with bupivicaine after careful neurological exam)
Femoral Shaft Fractures Definitive Management • Traction • no longer commonly employed • External fixation • especially open and comminuted fractures • Intramedullary rods • Operation of choice for most fractures • Has been shown to decrease hospitalization and total disability
Femoral Shaft FracturesDefinitive Treatment Bridging trabeculae 5 weeks post IM nail Callus formation 3 weeks post IM nail
Femoral Shaft FracturesComplications • Outcome generally good with close to 100% union rate. Potential complications include… • Malunion • Fat embolism • 2-23% of isolated femoral shaft fractures • Fever, tachycardia, ALOC, resp distress, petechiae • ARDS • Hemorrhage (average 1-1.5 litres) • Concurrent multisystem trauma • Limb-length discrepancy • Compartment syndrome of the thigh - rare
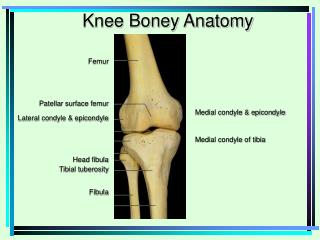
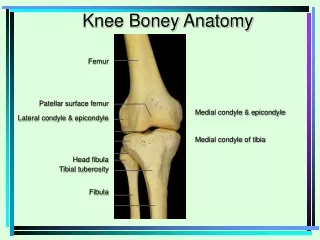
Knee Fractures • Distal Femur • Supracondylar • Intracondylar • Condylar • Patella • Proximal Tibia • Tibial plateau • Tibial spine
Ottawa Knee Rules • X-ray knees with knee injury and one or more of: • Blunt knee trauma in a patient >55 years old • Tenderness to palpation of head of fibula • Isolated tenderness of patella • Inability to flex knee to 90 degrees • Inability to bear weight both immediately and inability to take four steps in ED
Exclusion criteria • Isolated skin injuries • Referred patients from another ED or clinic • Injury >7 days old • Patient returning for re-evaluation • Distracting injuries • Altered mental status • Age < 18 years old • Pregnant patients • Paraplegia
Ottawa Ankle Rules • Derived from study of 1047 adult ankle injuries • 100% sensitive • 54% specific • Reduced radiography from 69% – 49% • Reduced time in ER by 39 minutes Stiell IG, Greenberg GH, Wells GA, et al: Prospective validation of a decision rule for the use of radiography in acute kneeinjuries. JAMA 275:611-615, 1996 Stiell IG, Wells GA, Hoag RH, et al: Implementation of the Ottawa knee rule for the use of radiography in acute kneeinjuries. JAMA 278:2075-2079, 1997
Knee Injuries • If Ottawa criteria are met x-ray: • AP / Lateral • “sunrise” view for patients with patellar tenderness • Oblique view / plateau view for patients unable to bear weight • provides better view of femoral condyles, tibial tuberosity, medial/lateral patellar margins • Tunnel view for patients with suspected ACL injury and tibial spine fracture
Pittsburgh Rules for Knee Radiographs Exclusion criteria • Injury >6 days old • Isolated skin injuries • History of knee fracture or surgery • Repeat visit for same injury
Pittsburgh vs Ottawa rules • More specific than Ottawa rules (60-80% vs 27-49%) • Comparable sensitivity (99% vs 97%) • One study found the Pittsburgh rules decreased knee radiography by 52% with one missed fracture vs 23% with three missed fractures Seaberg DC, Yealy DM, Lukens T, et al: Multicenter comparison of two clinical decision rules for the use of radiography in acute, high-risk kneeinjuries. Ann Emerg Med 32:8-13, 1998
Distal femur fractures • Uncommon • Result from high velocity trauma (MVC) • Hyperabduction • Adduction • Hyperextension • Axial loading • Extensive soft tissue injuries • Compartment syndrome - rare
Distal femur fractures • Examination • Knee pain • deformity • hemarthrosis • Supracondylar fractures • Shortened and externally rotated thigh • Quadriceps pull proximal fragment forwards • Gastrocnemius pulls distal fragment back
Femur fractures - imaging • AP • Lateral • Also don’t forget … • AP pelvis • AP/lateral hip
Distal Femur Fractures • Anatomy • Vascular • close to femoral/popliteal vessels • Assess distal pulses • Palpate for hematoma in popliteal fossa • Neurological • Tibial nerve – gastrocnemius, plantaris • Peroneal/Deep Peroneal nerves • Supplies anterior compartment (dorsiflexion) • Sensory to first dorsal interosseus cleft
Distal Femur Fractures • Supracondylar • Extra-articular • No hemarthrosis • Intracondylar • Intra-articular • Condylar • Intra-articular
Distal Femur Fractures • No definitive classification system • Evaluate based on • Displacement • Comminution • Soft-tissue injury • Neurovascular status • Joint involvement • Intra vs extra-articular • Open vs closed
Distal Femur Fractures • Complications – similar to femoral shaft • dvt • fat embolism • delayed union / malunion • valgus/varus deformities • chronic arthritis • compartment syndrome • growth disturbances in adolescents (65% of leg growth from distal femoral epiphysis!!)
Distal Femur Fractures • Management • assess & manage neurovascular status • analgesia (consider femoral nerve block) • immobilization • appropriate fluid management • orthopedic referral • definitive treatment (ORIF vs conservative)
Distal Femur Fractures Transcondylar fracture 10 months post ORIF
Patellar Fractures • Largest sesamoid bone in body • Acts to increase mechanical advantage during knee extension • 1% of all adult fractures • 27% occur during MVC’s – knee to dash • Most patellar fractures are intra-articular • Search for concomitant injuries • Knee/acetabular dislocations • Acetabular fractures • Femur fractures
Patellar fractures - mechanism • Indirect trauma • Forceful knee flexion against contracted quadriceps • Horizontal fractures common • Direct trauma • Direct blow / fall on knee • comminution
Patellar fractures - Px • Pain • Hemarthrosis • Crepitus • Disruption of extensor mechanism (must be able to fully extend knee against gravity)
Patellar fractures • Imaging • AP • Lateral • Sunrise • Tangential view across 45 degree flexed knee • Shows small vertical fractures of patella
Patellar fractures - Management • Nondisplaced with intact extensor mechanism • immobilize knee in extension with partial weight bearing x 3 weeks • Repeat x-ray in 3 weeks • Wear another 3 weeks for horizontal fractures, less for vertical fractures
Patellar Fractures Management • Displaced (>3mm bony separation or > 2mm articular surface disruption) • Orthopedic referral • Tension band / K-wires • Possible patellectomy – surgical connection of quadriceps and patellar tendons
Patellar Fractures 58 year old dashboard injury and comminution of patella
Patellar Fractures After total patellectomy and repair of the extensor mechanism
Tibial Fractures • Major load-bearing structure of lower leg • Thin overlying tissues • open fractures common • Easily fractured by direct trauma
Tibial Plateau Fractures • aka tibial condylar fracture • Mechanism - can be almost any … • axial compression • rotation • direct trauma • varus/valgus stress • Trivial mechanism in osteoporotic individuals • Very common after pedestrian vs automobile – due to valgus/varus stress
Tibial Plateau Fractures • Examination • Unable to weight bear • knee slightly flexed • knee effusion • Joint line pain • possible varus/valgus deformity (esp. with depressed fractures) • associated ligamentous and meniscal injuries • assess neurovascular status
Tibial Plateau Fractures • Imaging • if meets Ottawa rules • AP • lateral (medial condyle concave, lateral condyle convex) • if patient unable to weight bear 4 steps • oblique views • tibial plateau view (AP with 15 deg vertical orientation)
Schatzker Classification of tibial plateau fractures • 1. Lateral plateau fracture without articular depression • 2. Lateral plateau fracture with articular depression • 3. Isolated areas of lateral plateau depression NB: 60% are lateral plateau fractures (types I-III)