Download
1 / 13
130 likes | 350 Views
Visco Dissection. after phaco prechop. To facilitate the Phacoemulsification after Phaco Prechop. A Simple and Easy Procedure. Mitsui Memorial Hospital. Takayuki Akahoshi, MD. The author has no financial interest in the products introduced in this presentation. Introduction.

E N D
Visco Dissection after phaco prechop To facilitate the Phacoemulsification after Phaco Prechop A Simple and Easy Procedure Mitsui Memorial Hospital Takayuki Akahoshi, MD The author has no financial interest in the products introduced in this presentation.
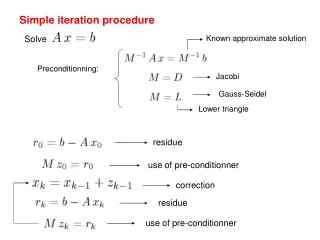
Introduction • Phaco Prechop is a procedure to divide the nucleus prior to the phacoemulsification. • If the nucleus is prechopped completely, the energy and time for the phacoemulsification can be remarkably reduced. • It is extremely helpful in the micro coaxial cataract surgery to protect the incision from the heat of the tip, corneal endothelium from the turbulence and optic nerve from the pressure. • The most important point in the Phaco Prechop is to attain the complete nuclear division. • The posteriorplate and periphery of the nucleus should be completely separated. • Visco dissection is an easy and simple procedure to attain complete separation of the nuclear fragments after Phaco Prechop.
Phaco Prechop • There are two methods in Phaco Prechop; Karate Prechop and Counter Prechop to be selected according to the lens pathology. • Required procedure before Phaco Prechop: • Fill up the anterior chamber with sufficient dispersive OVD. • Make a complete capsulorhexis. • Perform complete hydrodissection so that the nucleus can be rotated freely in the capsular bag.
Karate Prechop • Indication : Soft to medium nucleus with complete capsulorhexis and intact ciliary zonules. • Contra-indication : Hard nucleus, incomplete capsulorhexis and compromised ciliary zonules such as in pseudoexfoliation syndrome, post vitrectomized eye etc. If there is any difficulty to insert the prechopper blade into the nucleus, it is not a candidate for the Karate Prechop. • Instrument : Combo Prechopper, which has a sharp angular edge and blunt rounded blade is used. Combo II Prechopper which opens the blades wider through a smaller incision is most suitable for the sub-2mm micro coaxial surgery. • Method : After complete hydrodissection, the anterior chamber is filled with dispersive OVD. The angular edge of the Combo Prechopper is placed at the center of the nucleus. Insert the blade directly into the nucleus. The direction of insertion is just downwards. When the whole blade is inserted into the nucleus, open the blades slowly while pushing the nucleus downwards. Attain the complete division from the surface to the bottom, from proximal to the distal end of the nucleus. When the complete division has been attained, the inner surface of the posterior capsule can be observed. The rounded side of the blade is used to ascertain the complete division. Restore each bisected nuclear fragment into its original position, then rotate the whole nucleus 90 degrees to prechop it into 4 pieces, 60 degrees to 6 pieces.
Karate Prechop Vertical Prechop with a Combo II Prechopper
Counter Prechop • Indication : Medium to hard nucleus. Incomplete capsulorhexis or weak ciliary zonules. • Contra-indication : None. Contra-indication of the Karate Prechop is the indication of the Counter Prechop. Any kind of the nuclei can be prechopped either by Karate or Counter Prechop technique. • Instrument : Universal II Prechopper, which has a sharp slender blade will be used. To support the nucleus, Nucleus Sustainer (AE-2530) which has a micro ball at its tip can be safely used. For a myopic eye, sustainer with a longer tip (AE-2530L) is suitable to reach the equator of the nucleus. • Method : After complete hydrodissection, the anterior chamber is filled with dispersive OVD. The Nucleus Sustainer is carefully introduced under the capsulorhexis edge to the equator of the nucleus. The Universal Prechopper is inserted into the core of the nucleus. The tip of the sustainer, central core of the nucleus and the tip of the prechopper should be aligned on the same axis. Bring the sustainer towards the prechopper while holding the core of the nucleus with the two instruments. Then open the blades several times to prechop the nucleus. In case with a sclerotic hard nucleus repeat opening action until the posterior plate of the nucleus is completely separated. When the nucleus is completely prechopped from the surface to the bottom, from the proximal to the distal end, rotate 90 degrees using two instruments. Divide the nucleus into four pieces in the same way. Dispersive OVD can be injected several times to maintain the anterior chamber and clear the nuclear surface for better visibility. If the cortex may hinder the visibility of the nucleus, it can be aspirated before starting prechop. For the soft nucleus, prechopping into four pieces is enough to facilitate the following phacoemulsification. For the denser cataract, it is more advantageous to divide into six or eight smaller pieces.
Counter Prechop Horizontal Prechop with a Universal II Prechopper
Visco Dissection • Instrument : Visco dissection cannula can be hand-made by bending a G27 viscocannula using a needle holder.
Visco Dissection • Method : After prechop, inject the OVD into the space between the nuclear fragments and the capsular bag to separate each fragment from the bag.
Results • Effect on the aspiration time : There was no statistical difference between the dispersive and cohesive OVD in the Karate prechopped Grade II nucleus.
Results • Effect on the BSS consumption : There was no statistical difference between the dispersive and cohesive OVD in the Karate prechopped Grade II nucleus.
Results • Effect on the ultrasound energy : Visco dissection by cohesive OVD could reduce the CDE in the Karate prechopped Grade II nucleus.
Conclusion • Visco dissection by cohesive OVD can reduce the ultrasound energy in the phacoemulsification after Phaco Prechop. Reference • ”Phaco Prechop: Manual Nucleofracture Prior to Phacoemulsification” Operative Techniques in Cataract and Refractive Surgery, Vol. 1, No.2 1988: pp 69-91 • “Phacoemulsification Principles and Techniques” Second Edition, SLACK Incorporated, 2002: pp 333-346