Download
1 / 86
910 likes | 2.23k Views
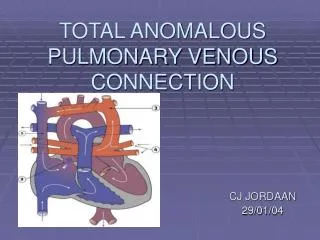
Pulmonary venous anomalies. Dolly mathew. Anatomy of pulm veins. Venous anomalies . Anomalous connections Anomalous drainage with normal connections Stenotic connections Abnormal number of pulmonary veins. Anomalous connections & drainage. TAPVC : all the veins connect anomalously

E N D
Pulmonary venous anomalies Dolly mathew
Venous anomalies • Anomalous connections • Anomalous drainage with normal connections • Stenotic connections • Abnormal number of pulmonary veins
Anomalous connections & drainage • TAPVC : all the veins connect anomalously • PAPVC : 1 or more, not all , of the veins connect anomalously • TAPVD/PAPVD: all or some of the pulmonary veins drain anomalously into the RA, without being abnormally connected Stenotic connections • Produce obstruction to pulmonary venous return to LA (N connection) / RA ( Anoconn)
Lungs,larynx,tracheobronchial tree – foregut • 27-29 days - lungbuds enmeshed in splanchnic plexus • End of 1st month- common pul vein – pul venous plexus & sinoatrial portion of the heart • Primary connections still patent
EMBRYOLOGIC CLASSIFICATION OF PUL VEN ANOMALIES 1-nl absorption of CPV assos with defects – in abnormal pulven drainage a) sinusvenosus defect b) malposition of septum primum 2-Early atresia of the CPV while PUL-SYST conn are still present a) PAPVC b) TAPVC 3-Late atresia after PUL-SYST connections are obliterated a) TAPVC 4- Stenosis of CPV a) cortriatriatum 5- abnormal absorption of individual pul veins into LA a) stenosis of individual pul veins b) abnormal no: of pul veins
Malposition of septum primum • When S2° absent, S1° displaced towards the anatomic LA • Incorporation of half or all of the pv into morphological RA • Normally connected pv drain into RA • Interatrial communication if S1° not reaching the post wall of LA ( sinus venosus defect)
PAPVC • Less than four pulmonary veins connected to RA or systemic vein(s) • Sex ratio is equal • Associations Asplenia and polysplenia Turner and Noonan ASD and TOF -Present in 9 % of ASDs. -Present in all cases of sinus venosus ASD Tricuspid atresia and single ventricle
PAPVC • RPVs to SVC – without abn connection • RPVs to IVC – more primitive anomaly • LPVs IVC • LPVs to LIV – veins from Lt upper lobe or whole Lt lung connect to LIV via vertical vein/ LSVC • Uncommon sites of PAPVC of LPVs to coronary sinus, Rt SVC, Lt subclavian , azygos vein
Scimitarsyndrome • Hypoplastic lung drained by an anomalous vein into systemic venous system (IVC , RA, portal vein) • PAPVC to IVC • Hypoplasia of right lung and • anomalies of bronchial system • Horseshoe lung • dextro position of heart • Hypoplasia of right pulmonary artery and abnormal systemic arterial supply to right lung • Pul sequestration
Scimitar syndrome synonyms • Pulmonary venolobarsyn • hypogenetic lung syndrome • Halasz’ssyn • mirror image lung syn • epibronchialrtpulm artery syn • venacavabronchovascularsyn
Associations • CHD- ASD, VSD,TOF, PDA • Ipsilateral diaphragmatic anomalies • Localisedbronchiectasis • Vertebral anomalies • Genitourinary tract abn
Treatment • Surgical correction – sig LR shunting ,PHTN • Interatrial baffle to redirect pvretrn to LA • Anomalous vein replanted directly into LA
Physiology PAPVC with intact IAS • Single pv – anomalous bld flow 20-25% TPBF • RA pressure < LA pressure • All but one pv – 80% TPBF ; phys & CF comparable with TAPVC PAPVC with ASD • PBF: SBF - 3.5: 1 • Bld from both lungs drained anomalously • Preferential shunting from rt lung in ASD more- proximity of rtpulm venous orifices to ASD
Clinical features • Cyanosis uncommon in childhood • Cyanosis during 3rd & 4th decades – changes in the pulmonary vascular bed, pulmonary HTN, increasing RL shunt
ECG • rR’ , rSR’ pattern • Peaked p , RVH – older patients with PHTN • CXR - increased pulmonary bld flow - RV dilation • Dilation of lower portion of SVC • Azygos vein- rounded bulge in rt sup mediastinum at rt heart border • LIV – snowman appearance of the mediastinum
Echo • RV vol overload in the absence of ASD – PAPVC MR angio & CT angio - diagnostic • Ideal - Wide field of view, excellent spatial orientation, unambiguous 3d delineation of the course, conn & drainage • Phase contrast cine MRI – quantifn of pvbld flow, determination of Qp/ Qs, flow to the rt or left lungs
Cardiac catheterization • Inability to pass Catheter from RA to LA or a difference between RA pressure and pulmonary wedge pressure – s/o PAPVC with intact IAS • Selective pulmonary angiography shows the anomalous pulmonary vein in levophase.
Management • Indications for surgery- • Qp/Qs more than 2:1 • Scimitar syndrome • Timing- 2 to 5 years
Sinus venosus defect • Atrial level shunt • Deficiency of common wall between Rt SVC & RUPV & RLPV • Unroofing of PV into SVC or RA • Closure of defect between svc & rpv • Enlargement of interatrial communication& baffling rpvs to LA via enlarged comm used for rtatrialsv defects
TAPVC • TAPVC - all four pulmonary veins drain directly or indirectly into the right atrium • INCIDENCE- rare ( 4/1000 cases) • 1.5- 3% of CHDs • no sex predliction (males in TAPVC to portal vein) • Asplenia, polysplenia , cat’s eye syndrome • ASD/ PFO necessory to sustain life
DARLING’s classification type 1- conn at supracardiac level type 2- at cardiac level ( coronary sinus) type 3- at infracardiac level type 4- at two /> of the above levels • SMITH classification supracardiac ( without pulven obstruction) Infradiaphragmatic(with pulven obstruction) • Burroughs Edwards classification Long, intermediate, short
Supracardiac (45%) lt vertical veinLIV / SVC / azygos • Cardiac (25%)to CS / RA • Infracardiac (25%) portal vein, ductusvenosus, hepatic vein, IVC • Mixed (5%)lt lung to lt vertical vein, remainder of both lungs to CS
Supracardiac TAPVC to LIV infradiaphragmatic to portal vein
ANATOMIC SITES OF OBSTRUCTION TO PUL VEN DRAINAGE • nearly all- infra card, 65% svc, 40% LIV , 40% mixed • Obstruction at the level of interatrial septum • Obstruction in the anomalous venous channel intrinsic narrowing TAPVC supracardiac - jn of Lt vv to LIV / HVC / SVC TAPVC to CS – ostium, jn of CPS & CS Infracardiac – jn of connecting vein to portal vein/ ductusvenosus - penetrates diaphragm -ductusvenosus undergoes constriction- drainage obst
extrinsic pressure - vertical vein to LIV passing bet L main pul art & L main stem bronchus – vascular vise - TAPVC to SVC - RPA & trachea -to portal vein- hepatic sinusoids interposed, results in inc resistance to venous return
TAPVC without pv obstruction • The mixed venous pool receives 3-5 parts of fully saturated blood for each part of systemic venous blood • RA saturation ≥ 90% • Progr RV hypertrophy & dilation • TAPVC with pvo • Elevated pressure in the pv channels freely transmitted to capillary bed • Osmotic pressure of blood > hydrostatic pressure in the capillaries pulm edema • RV vol & pr overload, decreased LV vol, low systemic output
Hemodynamic considerations • Severe pvobstrn – pv HTN – pulmlymphangiectasia • LA/ LV small – lack of pv drainage to LA • Narrowing of aortic isthmus & CoA
After birth • Pv severely obstructed, pulmbld flow reduced & if systemic flow is maintained, pulm to syst flow ratio decreases, arterial O2 sat falls • Unobstructed pv – as PVR falls, pulmbld flow increased – high pulm to syst flow ratios – high syst o2 saturations
PVR & pulmbld flow • Fall in PVR -↑pulmbld flow - ↑flow in PVs- if veins obstructed, pulm venous pressure elevated • If plasma oncotic pressure exceeded , transudation of fluid - pulmoedema
Role of foramen ovale • In the absence of pulmonary venous return to LA, RA pr > LA pr, R L flow thru foramen ovale • Severe obstruction – large foramen ovale- provide adequate systemic bld flow without significant elevation of RA pressure • Restriction of foramen ovale with moderate – no PVO
Role of ductusarteriosus • As PVR high, bld shunts from PA Ao thru ductus ↓flow thru’ pulmonary circulation • Pulm venous flow ↓, pulm venous pr ↓, less likely pulm edema • Ductus closes – RL shunt eliminated – PA pr & lung perfusion ↑- pulm venous flow, pr & pulm edema ↑
Role of ductusvenosus • Pulm venous bld returning to portal vein IVC • Pulm venous HTN & pulm edema will not dev • Closure of ductus flow thru’ hepatic microcirculationportal , pv pressure ↑- pulm edema
Effect of feeding • ↑gastrointestinal & portal flow • Portal & pulm venous pr will rise – pulm edema aggravated
Effect of PGE1 infusion • -Dilating the ductus - ↑ RL shunt , ↑ cyanosis - Pulm vasodilatation, ↑pulmbld flow, ↑pulm edema, improve cyanosis • Beneficial – infra diaphragmatic • Relaxes smooth muscle in ductusvenosus & relieves constriction- lower the pulm venous pressure – improvement of pulm edema
Natural history • Assymptomatic at birth • 56% syptomatic at 1st month of life • Failure at 6months of age • Severe obstrn- pulm edema 1st few hrs • Cyanosis mild, more with failure & pulm vascular changes
Natural history • Death – 1st few wks or months of life in most neonates • 90% death – 1st year of life • Survivors of 1st few wks of life – incrpulmbld flow mild cyanosis, PHTN • 50% survive beyond 3/12 • 20% surviving the 1st yr • Median survival 3wks (obst) , 2.5 months in (non obstr) • Infracardiac- worse prognosis- 3wks survival
Pulses – weak, BP reduced, small pulse pr • Prominent RV heave • Loud s1, s2 wide fixed split , loud p2, s3 at apex,s4 frequently in older patients • Cont mr if Lt vertical vein obstructed • 2/6 soft blowing systolic mrpulm area ( turbulence in the pulm outflow tract) • TR murmur at LLSB
ECG- RA enlargement , RAD,RVH • CXR- RA, RV enlarged • PA segment prominent • Figure of 8 or snowman – TAPVC to LIV • Lung fields reflect increased pulmbld flow
Echo PVs are farthest from the transducer (most posterior structures) • RA/RV vol overload • LV vol decreased • Pulm venous confluence & individual pv imaged • Cs dilated, if TAPVC conn to cs
Left superior LA Left inferior Ao LAA Normal Pulmonary Veins Often, at least three pulmonary veins can be seen in the parasternal short axis views by subtle adjustments in the transducer postion.