Download
1 / 28
290 likes | 543 Views
HRS/EHRA/ECAS Consens us Statement on Catheter and Surgical Ablation of Atrial Fibrillation. K.R. Julian Chun. Asklepios Klink St. Georg, Hamburg. ACC/AHA/ESC 2006 Guidelines for the Management of Patients with Atrial Fibrillation. Fuster et al. Circulation 2006;114: 257-354.

E N D
HRS/EHRA/ECAS Consensus Statement on Catheter and Surgical Ablation of Atrial Fibrillation K.R. Julian Chun Asklepios Klink St. Georg, Hamburg
ACC/AHA/ESC 2006 Guidelines for the Management of Patients with Atrial Fibrillation Fuster et al. Circulation 2006;114: 257-354
Catheter ablation of atrial fibrillation SUCCESS RATES Verma A et al. (Circulation 2005;112:1214–1231)
Catheter ablation of atrial fibrillation COMPLICATIONS – LARGE Centers Pooled data complication rate: 2.8% Verma A et al. (Circulation 2005;112:1214–1231)
Catheter ablation of atrial fibrillation COMPLICATIONS - World Wide Survey % n= Cappato et al. Circulation 2005; 111; 1100-1105
7.0 6.0 5.0 4.0 3.0 2.0 1.0 0 Prevalence Atrial Fibrillation 5.61 5.42 5.16 4.78 4.34 3.80 Adults with atrial fibrillation [millions] 3.33 2.94 2.66 2.44 2.26 2.08 1990 1995 2000 2005 2010 2015 2020 2025 2030 2035 2040 2045 2050 Year Go et al, JAMA 2001;285:2370
HRS/EHRA/ECAS Consensus Statement Definitions Atrial Fibrillation (AF) • Paroxysmal AF: AF (≥2 episodes) that terminates spontaneously within 7 days • Persistent AF: >7 days or cardioversion • Longstanding persistent AF: >12 months continuous AF • Permanent AF: AF has been accepted Heart Rhythm. 2007 Jun;4(6):816-61.
HRS/EHRA/ECAS Consensus Statement Mechanisms of Atrial Fibrillation Heart Rhythm. 2007 Jun;4(6):816-61.
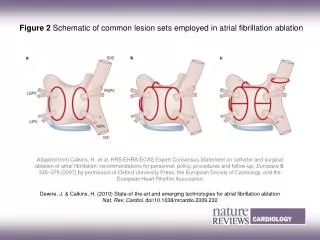
HRS/EHRA/ECAS Consensus Statement AF Ablation Strategies Heart Rhythm. 2007 Jun;4(6):816-61.
AF Ablation Strategies Heart Rhythm. 2007 Jun;4(6):816-61.
CFAE Definition Haissaguerre et al. JCE 2005
HRS/EHRA/ECAS Consensus Statement Heart Rhythm. 2007 Jun;4(6):816-61.
Procedural Endpoint Ouyang et al. 2004 Circulation Heart Rhythm. 2007 • Wide area circumferential lesions (CCL) • Online Lasso recordings to prove PVI
#9 #1 #7 #4 #1 #9 #7 #4 Lateral PVs
Pulmonary Vein Isolation LSPV LIPV His Map CS LSPV LAA LIPV Ouyang F et al. (Circulation 2004;110:2090–2096)
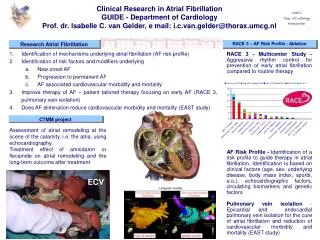
HRS/EHRA/ECAS Consensus Statement Indications for AF Catheter Ablation • It is important to recognize that catheter ablation of AF is a demanding technical procedure that may result in complications • Patients should only undergo AF ablation after carefully weighing the risks and benefits of the procedure Heart Rhythm. 2007 Jun;4(6):816-61.
HRS/EHRA/ECAS Consensus Statement Indications for AF Catheter Ablation • Symptomatic AF refractory ≥ 1 AAD (Class I, III) • AF ablation as first line therapy (rare clinical situations) • Selected pts with heart failure and/or reduced EF Heart Rhythm. 2007 Jun;4(6):816-61.
HRS/EHRA/ECAS Consensus Statement Complications in AF Ablation • Cardiac tamponade (<6%) • Pulmonary vein stenosis (0-38%) • Atrio-Esophageal fistula (<0.25%) • Phrenic nerve injury (<0.48%) • Thromembolism (0-7%) • Post procedural arrhythmias (5-25%) • Vascular complications (0-13%) • Radiation exposure Heart Rhythm. 2007 Jun;4(6):816-61.
HRS/EHRA/ECAS Consensus Statement Technique / Lab Managements • Heparin Target ACT 300 to 400s • Careful identification of PV ostia is mandatory • If additional lesions are applied, line completeness should be demonstrated • RAI block only in pts with typical or inducible AFL • Non PV triggers should be targeted if possible • If pts with longstanding persistent AF are approached, ostial PVI may not be sufficent Heart Rhythm. 2007 Jun;4(6):816-61.
HRS/EHRA/ECAS Consensus Statement Minimal Monitoring • F/U visits; 3 months, 9 months and then every 6 months for at least 2 years • Event monitor in pts who complain of palpitations • AF/AFL/AT >30s are treatment failures • 24h HOLTER is acceptable for minimal monitoring for pts in clinical trials and is recommended at 3 to 6 months intervals for 1 to 2 years Heart Rhythm. 2007 Jun;4(6):816-61.
Hamburg AF Ablation Approach • 1. Procedure: Wide area circumferential PVI of ipsilateral PVs • 2. Procedure: Re-check PV conduction: Gap closure • Clinical AT Ablation • 3. Procedure: CFAE identification and ablation (LA, CS, RA) • Clinical AT Ablation
HRS/EHRA/ECAS Consensus Statement Conclusion • Catheter ablation of AF is... • performed throughout the world • associated with high success rates • significant complications • PV isolation is cornerstone of AF ablation