Download
1 / 39
510 likes | 1.93k Views
Salivary Gland Disorders. Salivary Gland Disorders ENT for the PA-C. Andrew Golde MD,CM FRCSC FACS Advanced Ear, Nose and Throat Associates Atlanta, GA February 2011. Classification of Salivary Disorders. Infections Systemic disorders Trauma Medication side-effects Neoplasms.

E N D
Salivary Gland DisordersENT for the PA-C Andrew Golde MD,CM FRCSC FACS Advanced Ear, Nose and Throat Associates Atlanta, GA February 2011
Classification of Salivary Disorders • Infections • Systemic disorders • Trauma • Medication side-effects • Neoplasms
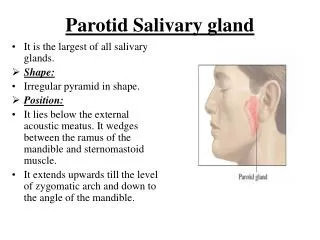
Salivary Gland Anatomy • Major salivary glands • Parotid (2) • Submandibular (2) • Sublingual (2) • Minor salivary glands (5000)
Salivary Gland Physiology • Autonomic control • Parasympathetic ---> secretion (Ach) • Sympathetic ---> composition (adrenergic) • Complex composition • Electrolytes, urea, ammonia, glucose, cholesterol, fatty acids, lipids, amino acids, proteins (albumin, globulin, enzymes, glycoproteins, polypeptides including kallikrein, epidermal growth factor, renin, glucagon, angiotensin II, erythropoetin, gastrin, somatostatin)
Functions of Saliva • Lubricant • Aid swallowing, mechanical cleaning • Digestion • Enzymatic cleavage - amylase • Mediation of taste • Excretion • Blood group proteins, mediators, viruses • Defense • Antibodies, mucosal integrity
Saliva Production • Max rate 1 ml/min/gm of tissue • High blood flow (10x equal mass muscle) • Distribution • Parotid 75% low viscosity • Submandib 20% medium • Minor 5% high
Take Home Message • Three categories of problems • 1. Altered saliva production • 2. Painless swelling of saliva glands • 3. Painful swelling of saliva glands
Disorders of Altered Physiology • Increased or decreased stimulation • Medication, neurogenic, hormonal • Obstruction of secretion • Sialadenitis, sialolithiasis • Change of composition • Cystic fibrosis • Nutrition • Parenchymal damage • Irradiation, Sjogren’s syndrome, cystic fibrosis
Sialadenosis • Recurrent painless swelling (parotid) • Etiology • Endocrine disorders (diabetes) • Malnutrition (protein, ETOH, vitamin) • Autonomic dysfunction • Treatment • Correct underlying causes • Reassurance
Sialolithiasis • Formation of salivary stones • Submandibular (92%) > Parotid (6%) > Minor (2%) • High mucin content, Alkaline pH, high concentration organic matter and Ca and salts • Anatomy of Wharton’s duct • One of most common causes of salivary dysfunction
Sialolithiasis • Etiology • Enhanced in presence of stasis of salivary flow • Genetic predisposition (kidney stones, gout) • Mineralization of a mucoid gel • Clinical Presentation • Asymptomatic • Recurrent swelling associated with eating • Spitting out stones • Sialadenitis (infection)
Sialolithiasis • Management • Hydration • Massage (Post --->Ant) + heat • Anti-inflamatories • Antibiotics if infected • Removal of stones • Sialendoscopy • Surgical excision of affected gland
Disorders of Decreased Saliva • Irradiation • Sjogren’s syndrome • Cystic fibrosis • Anti-cholinergic side effects of meds
Irradiation of Salivary Glands • Conventional XRT for head and neck tumors 6000-7000cGy over 6-7 weeks • 50% function lost after 1000 cGy • 90-100% loss after complete course of XRT • Xerostomia can last for several years • Loss of taste • Increased incidence dental carries • Altered nutritional status • Loss of appetite
Irradiation of Salivary Glands • Protective strategies • IMRT (Intensity modulated radiation therapy) • Lower total doses (Canada vs US) • Amifostine • Free oxygen radical scavenger • Difficult to tolerate • Treatment • Supportive - H2O, lubricants • Salivary promoting drugs
Sjogren’s Syndrome • Autoimmune disease of major and minor salivary, lacrimal, mucous and sweat glands • 1933 Sjogren original description • Keratoconjunctivitis sicca • Xerostomia • Rheumatoid arthritis (scleroderma, mixed connective tissue disease, polyarteritis nodosa, polymyositis, SLE) • Classification • Primary - Sjogren’s syndrome alone • Secondary - Sjogren’s plus other autoimmune
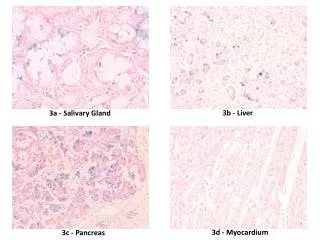
Sjogren’s Syndrome • Diagnosis • Lower lip minor salivary gland biopsy • Dense lymphocytic infiltrate/plasma cells • Sjogren’s autoantibodies • Positive Rheumatoid factor • Elevated C-reactive protein • High titers IgA, IgG, IgM • Demographics • Female >> male • Middle age
Sjogren’s Syndrome • Treatment • Artificial lubricants for ocular, nasal and oral dryness • Salivary stimulants (Evoxac) • Immunosuppressants (Plaquenil, MTX, Humara) • Predisposition to Non-Hodgkin’s lymphoma • Parotid gland mass enlarging (painless) • MALToma
PAINLESS Sialadenosis Sialolithiasis Sjogren’s HIV Granulomatous Benign primary tumors Lymphoma PAINFUL Bacterial sialadenitis Mumps Malignant primary tumors Swelling of Saliva Glands
Salivary Infections • Primary bacterial (sialadenitis) • Secondary viral • Granulomatous
Sialadenitis • Bacterial infections of salivary glands • Mechanical blockage of salivary ducts or reduced production of saliva • Retrograde contamination by oral cavity flora • Classification • Acute • Recurrent • Chronic
Acute Sialadenitis • All glands - parotid most frequent • Contributing factors • Stasis; immunocompromise; poor oral hygiene • Post-op • Dehydration • Anti-cholinergics or diuretics • Rapid onset pain, swelling, induration • Suppurative discharge from duct • S.aureus, S. pyogenes, S. viridans, S. pneumoniae, H. flu
Acute Sialadenitis • Treatment • B-lactam resistant penicillin or cephalosporin • Augmentin, Clindamycin • Steroids • Fluid replacement • Sialogogues • Analgesics • Manual massage • Topical heat
Recurrent Sialadenitis • Mechanical obstruction most common factor • CT scan of neck with contrast to rule out stones or intrinsic lesions or abscess pockets • Oral anaerobes prominent • Clindamycin, Augmentin, Flagyl + ceph, Avelox • Surgical excision of gland as last resort
Chronic Sialadenitis • Usually follows recurrent infections • Permanent alteration of gland architecture • Surgical excision required
Acute Sialadenitis • Complications include abscess • Persistent symptoms > 4 days of Rx • Uni or multiloculated • CT scan of neck with contrast • Sialography contraindicated • Surgical drainage
Secondary Viral Infections • Hematogenous dissemination • Mumps • HIV
Mumps • Single most common cause of acute nonsuppurative sialadenitis in childhood • Bilateral parotid swelling (+++) • Rarely submandibular • Pain exacerbated by eating • Paramyxovirus • Highly contagious - airborne droplets • Incubation 18 days • MMR vaccination
Mumps • Diagnosis is clinical • Hemagglutination inhibition or complement fixation • Elevated serum salivary type amylase • Viremia abates in 7 days • Gland swelling abates in weeks • Hydration and rest • Severe cases • Meningoencephalitis, orchitis, pancreatitis, nephritis • Other viruses rarely mimic • Parainfluenza, coxsackie, echovirus, EBV
HIV Infection • HIV-SGD: HIV-associated salivary gland disease • Parotid glands most commonly affected • Gradual painless cystic enlargement • Xerostomia, xerophthalmia, arthralgias • Cysts up to several cm in size • Originate within lymph nodes • 10% coexistence of lymphoma • CT scan and FNA if suspicious • Surgical excision if considering lymphoma diagnosis
Granulomatous Infections • Not uncommon • Painless gradual enlargement of isolated mass in gland • DDX includes neoplasm • Etiology • Typical and atypical TB • Actinomycosis • Cat scratch • Toxoplasmosis • Tularemia • CT scan, FNA, serology
Salivary Gland Tumors Benign vs. Malignant Neoplasms
BENIGN Painless Slow growing Facial nerve intact More common MALIGNANT Can be painful Growing rapidly Facial nerve can become paralyzed Lymphadenopathy Less common Salivary Gland Tumors
Location of Gland Parotid Submandibular Minor Incidence of Malignancy 20% 50% 80% Salivary Gland Tumors
Benign Salivary Tumors • Adenomas • Pleomorphic • Monomorphic • Wathin’s tumor • Oncocytoma • Oncocytic papillary cystadenoma • Myoepithelioma • Sialadenoma • Inverted ductal papilloma • Hemangioma • Lymphangioma
LOW GRADE Mucoepidermoid ca Acinic cell ca Adenocarcinoma HIGH GRADE Mucoepidermoid ca Adenoid cystic ca Adenocarcinoma Carcinoma ex pleomorphic Squamous cell ca Undifferentiated ca Malignant Salivary Tumors
Factors Influencing Survival • Histopathologic diagnosis • Lymph node metastasis • Pain • Facial nerve paralysis • Skin involvement • Stage • Location • Recurrence • Distant metastases
Evaluation of Suspected Tumors • FNA • CT scan of neck with contrast • Surgery for frozen section analysis