Download
1 / 45
490 likes | 955 Views
Gastrointestinal Diseases and Disorders. Karen E. Hall, M.D., Ph.D. GRECC, Ann Arbor VA Health System University of Michigan Health System. Contributors to GI chapter: George Triadafilopoulos, MD Annette Medina-Walpole, MD William J. Hall, MD. Purpose. Handouts.

E N D
Gastrointestinal Diseases and Disorders Karen E. Hall, M.D., Ph.D. GRECC, Ann Arbor VA Health System University of Michigan Health System Contributors to GI chapter: George Triadafilopoulos, MD Annette Medina-Walpole, MD William J. Hall, MD
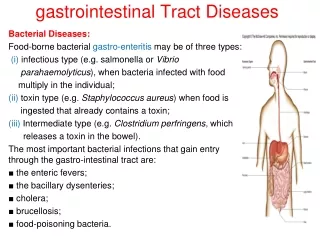
Proximal and distal GI tract at greatest risk for dysfunction with aging
Reflux risk increases with age LES pressure decreases with age: Gastroesophageal reflux disease (GERD)
Achalasia Subset of patients have pathologic increase in LES pressure: Female: Male 4:1 Age 75-85 years Progressive dysphagia to liquids and solids
Achalasia LES: “Bird’s beak” LES normally closed at rest Relaxation impaired: inhibitory NO and VIP neurons absent or dysfunctional
Achalasia Treatment Forcible balloon distension Rupture, mediastinitis, sepsis Botulinum toxin injection Relief x weeks-months ?Frail - high risk for balloon Laparoscopic LES myotomy ?similar risk/benefit as balloon
Splanchnic blood flow decreases with age Upper GI tract and proximal small bowel protected due to rich anastomotic supply Decreased blood flow to liver: Impaired metabolism: drugs, bilirubin “Watershed” areas at risk for ischemia (colon)
Diverticular disease: ?Western Aging Circular muscle: fewer fibers; larger spaces between fibers Colonic collagen increases in thickness with aging: Prolongation of muscle contraction Intraluminal pressure increases Mucosa/submucosa protrudes through wall = diverticulum
Aging sets the stage for clinical impairment Physiologic effects of aging + Superimposed disease Effects of medications = Clinical impairment in areas already at risk due to normal aging
Barrett’s Esophagus Mucosa: Squamous to intestinal Pre-malignant: Dysplastic foci require biopsy for detection High grade dysplasia (HGD) has significant risk of progression to adenocarcinoma
Barrett’s Esophagus • Earlier studies: • 7-10% risk of adenocarcinoma per year? • Up to 1998-99: • 1. Screening EGD for patients with GERD history • +Barrett’s: biopsy HGD: surgical referral • Low-Moderate Grade Dysplasia: high dose PPI • Follow-up EGD every ? 6 months – 1 year?
Should we treat Barrett’s Esophagus? Recent RCTs of proton pump inhibitor treatment: No significant effect on: Rate of progression of low-moderate dysplasia to HGD Rate of esophageal adenocarcinoma Screening EDG: esophageal cancer in 3%
Should we treat Barrett’s Esophagus? Why didn’t PPI treatment work? ? Not long enough (6 mo – 2 years) ? Genetic mutation already present ? Acid exposure not the only cause ? Biopsy error
Should we treat Barrett’s Esophagus? • Current recommendations: • 1. Screening EGD for patients with GERD history • 2. +Barrett’s: biopsy +for HGD: surgical referral • M-LGD: ?PPI + Follow-up EGD ?timing • Watch for future developments