Download
1 / 22
220 likes | 331 Views
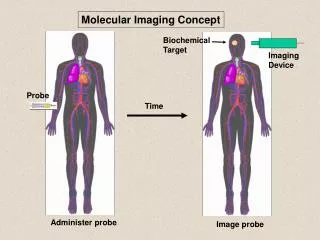
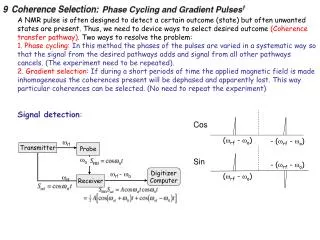
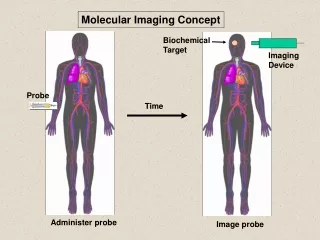
Prostate probe with SPECT technique NSS – MIC 2010 - November 5 - Knoxville F. Garibaldi- INFN – Roma1 – gr. Coll. ISS . the medical problem the proposal Layout Multimodality SiPM/electronics summary and outlook. Patient injected with radioactive drug.

E N D
Prostate probe with SPECT technique NSS – MIC 2010 - November 5 - Knoxville F. Garibaldi- INFN – Roma1 – gr. Coll. ISS • the medical problem • the proposal • Layout • Multimodality • SiPM/electronics • summary and outlook
Patient injected with radioactive drug. Drug localizes according to its metabolic properties. Gamma rays, emitted by radioactive decay, that exit the patient are imaged. Radionuclides imaging techniques • Collimator • Only gammas that are perpendicular to imaging plane reach the detector • Readout Electronics • Amplify electrical signal and interface to computer • Scintillator • Converts gammas to visible light • Computer decoding procedure • Elaborate signal and gives image output • Photodetector • Convert light to electrical signal
Compton Camera mechanical collimation PET Multi pinhole
Single photon techniques pros • simple(r) • cheape(r) • extending the radiotracers available • dual tracer looking at two different biological processes cons • - efficiency • spatial resolution
Compton Prostate Imaging Probe Internal Compton Probe External Compton Probe
Predicted Internal Probe Performance 141keV 511keV 171keV 245keV 364keV 4mm Point-to-Point, 1cm from probe (Monte Carlo simulation + ML reconstruction) Comparison with SPECT for In-111
Organ Relative Uptakes Prostate 1.0 Liver 2.0 Blood 1.5 Bone 0.7 Kidney 1.0 Spleen 1.0 Bladder 0.6 Rectum 0.4 Testes 0.6 Relative Uptake of In-111 Prostascint Averaged from three In-111 Prostascint SPECT scans
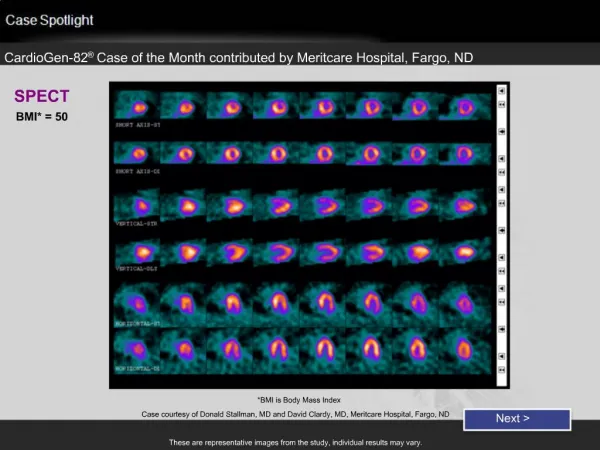
Conventional SPECT Reconstructions 5:1 10:1 15:1 20:1 w / tumor Prostate bkgd 171 and 245 keV, 8.8M events / 40 slices Spatial resolution ~15mm FWHM
Compton Prostate Probe Reconstructions 245 keV only, 1.2 million events, 8mm lesion Prostate 5:1 10:1 15:1 20:1 w / tumor bkgd Spatial resolution ~2mm FWHM
Internal Detector Details 10–12 layers of 1mm thick Si detectors + position and orientation sensor Exploded View Assembled Unit
Compton Probe Promising but Challenging • First detector • Energy resolution – largely addressed • Timing resolution – still an issue • Packaging – solvable • Second detector • Countrate capability – solvable • Cost – always an issue • System • Image reconstruction – solvable
Detector Packaging Use Tape Automated Bonding (TAB) (Very thin kapton tape with aluminum traces) Kapton microcables “Raw” energy spectrum Detector VATA ASIC Unfolded energy spectrum Kapton “hybrid” board
Timing • Desired time resolution <10ns FWHM • Poor timing from Si is evident • Slower signal generation from events near backplane • Large range of pulse-height coupled with leading-edge trigger is a big issue time-walk • Signal generation depends on 3D interaction position and recoil electron direction time-jitter BGO-Silicon timing spectrum for 511 keV source Signal generation at two biases for three depths
How Challenges Affect Performance • Consider anticipated countrate with In-111 Prostascint (from Monte Carlo simulations): • ~4 Mcps on second detector • ~40 kcps on scattering detector • 50 ns time window for present Si detectors (may need to be even larger) • Crandom= 2 x 4x106 x 4x104 x 50x10-9 = 16,000 cps ! • Ctrue was only ~10 kcps (or less) • Performance dominated by randoms! • Energy sum window can be used to reject randoms but only if the second detector also has good energy resolution
External Multipinhole Alternative • External probes will have small FOV and limited-angle tomography but… • SPECT/CT can identify prostate region • Probe can be computer-steered to image desired FOV • Conventional SPECT can be used to “complete” probe data
Endorectal Multipinhole? 30mm ~15mm • Some tomographic capability • Requires high detector resolution (0.5–1 mm + depth-of-interaction) • High enough efficiency and resolution?
Radionuclides Single photon • 111In-ProstaScint is not a good radiotracer but a new one proposed by M. Pomper looks promising. The single photon endorectal probe provides 2D imaging. We have to try to have 3 D images ( using multipinhole collimation and/or adding up a SPECT tomograph (spatial resolution would be dominated by the small probe (see later, the PET case))
our proposal -insert scintillator pixels into square holes of the collimator better performances (spatial resolution (?) and sensitivity (thicker scintillator)) -using diverging collimator better performances (reducing scan time) -using multipinhole collimation better performances (increasing sensitivity, tomographic recinstruction)
New radiotracers coming soon (M. Pomper , Johns Hopkins) Radiotracers available for SPECT and PET (from “New agents and Techniques for Imaging prostate cancer” A. Zahreer, S. Y. Cho, M. Pomper”, to be published on JNM) SPECT: Prostascint, Bombesyn,99mTechnetium nanocolloid (limphonodes), other coming soon… PET C—11 Choline, F-18-Choline, Ga-68 Dotabomb (Hofmann (Rome workshop)) many others coming… (collaboration with Johns Hopkins for testing in ISS (mice models for prostate available) and/or at JHU)