Download
1 / 12
341 likes | 957 Views
MEASUREMENT UNCERTAINTY. Dr A A KHINE DIVISION OF CHEMICAL PATHOLOGY NHLS TYGERBERG STELLENBOSCH UNIVERSITY Laboratory Management workshop 3-6 June 2019. MEASUREMENT UNCERTAINTY.

E N D
MEASUREMENT UNCERTAINTY Dr A A KHINE DIVISION OF CHEMICAL PATHOLOGY NHLS TYGERBERG STELLENBOSCH UNIVERSITY Laboratory Management workshop 3-6 June 2019
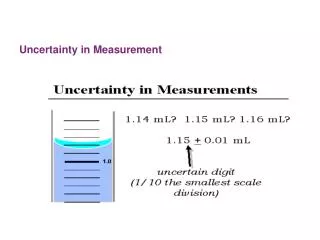
MEASUREMENT UNCERTAINTY is a parameter, associated with the result of a measurement… that defines the range of the values that could reasonably be attributed to the measured quantity (UKAS) Non-negative parameter characterizing the dispersion of the quantity values being attributed to a measurand, based on the information used.
MU is requirement in ISO standards and accreditation • ISO 15189:2012: • “The laboratory shall determine measurement uncertainty for each measurement procedure in the examination phases used to report measured quantity values on patients’ samples. The laboratory shall define the performance requirements for the measurement uncertainty of each measurement procedure and regularly review estimates of measurement uncertainty.”
Steps of the evaluation of the measurement uncertainty Time Scale BMICH
Approaches in estimating MU Definition of the Measurand Single laboratory Inter laboratory Component by Component Evaluation ISO GUM Single lab Validation Within-lab reproducility & Bias NordTest Interlaboratoy Validation Reproducibility and Bias ISO 5725 ISO TS 21748 Proficiency Testing (PT) Between Lab Variability ISO Guide 43 ISO 13528 BMICH
ISO 15189 gives some guidance • The relevant uncertainty components are those associated with the actual measurement process, commencing with the presentation of the sample to the measurement procedure and ending with the output of the measured value. • Measurement uncertainties may be calculated using quantity values obtained by the measurement of quality control materials under intermediate precision conditions that include as many routine changes as reasonably possible in the standard operation of a measurement procedure, e.g., changes of reagent and calibrator batches, different operators, scheduled instrument maintenance BMICH
Based on assumption approach- uses imprecision from long-term IQC See NHLS QA UOM sheet Hierarchical judgement of performance- desirable, minimum and maximum analytical goals- from CVi or CVw from BV database (Westgard), then CEC endorsed CV limits When the analyte is not in the BV list, search from other sources such as RCPA, drgrhodes Optimum: CVA = < 0.25 x CVI Desirable: CVA = < 0.50 x CVI Minimum: CVA = < 0.75 x CVI • Optimum: BA = < 0.125 (CVI2 + VG2)1/2 • Desirable: BA = < 0.250 (CVI2 + CVG2)1/2 • Minimum: BA = < 0.375 (CVI2 + CVG2)1/2
Why do we estimate MU? • Reference change values (RCVs) • Determines whether the difference between two results is negligible due to uncertainty or significant due to a genuine change in the condition of the patient. • RCV = 2.77 x √(CVA2 + CVI2) • Compare the MU and RCV to make medical decisions (but your performance must be acceptable first before you use the MU in this way) • Look at Performance Index (CVa/CVi or w) • if <0.5 – performance is acceptable • If < 0.75 – still okay • if > 0,75 – not acceptable (in this case do not report the MU, in fact so not release results. Stop testing and troubleshoot – check if you have trim out the IQC data when you print the 6 monthly data
Should we report it on the patient’s result? • Different opinion • What does NHLS say? • What does ISO say? • What are peers doing? • When should we report MU and when we should not?