Download

1 / 32
360 likes | 1.01k Views
Introduction to TPN. 新光吳火獅紀念醫院 內科部 胃腸肝膽科 柯威旭 醫師. Nutrition Support Team. Physicians Clinical pharmacists Nurse-Clinicians Dietitians Laboratory research technician Ward nursing staff In SKH: 主任 , 執行秘書 , 各科醫師 , 藥劑師 , 營養師. Source of Nutrition. Enteral nutrition Parenteral nutrition

E N D
Introduction to TPN 新光吳火獅紀念醫院 內科部 胃腸肝膽科 柯威旭 醫師
Nutrition Support Team • Physicians • Clinical pharmacists • Nurse-Clinicians • Dietitians • Laboratory research technician • Ward nursing staff • In SKH:主任,執行秘書,各科醫師,藥劑師,營養師
Source of Nutrition • Enteral nutrition • Parenteral nutrition • Central parenteral nutrition (CPN=TPN) • Peripheral parenteral nutrition (PPN) • Long-term home parenteral nutrition (HPN)
Clinical decision algorithm route of nutrition support Nutrition Assessment Decision to institute specialnutrition support YES NO Functional GI Tract Enteral Nutrition Parenteral Nutrition Short-term: NG, ND,NJ Long-term: Gastrostomy Jejunostomy GI function TPN PPN Intact Nutrients Defined Formula GI function return Adequate Inadequate Adequate YES NO PN Oral Feeding
PPN • High risk of thrombophlebitis • Osmolarity: less than 800-900 mOsm/kg • Short-term: up to 2 weeks • Not the optimal choice for • significant malnutrition • severe metabolic stress • large nutrient or electrolyte needs (especially potassium, a strong vascular irritant) • fluid restriction • the need for prolonged intravenous nutrition support
Indications of TPN • Impossibility for enteral nutrition • Inadequacy for enteral nutrition • Increment of the severity of disease by enteral nutrition PLUS • Anticipated to have PN for more than 7 days
TPN in Internal Medicine • Acute pancreatitis • Intestinal disease (IBD, NEC, radiation colitis, ileus, intractable diarrhea / vomiting) • Cancer • Hepatic failure • Renal failure • Short bowel syndrome • Enterocutaneous fistula • AIDS • Perioperative support
TPN should not be used in • Malignancy: poor response to R/T or C/T • Active stage of IBD • Relative preserved GI function • Hypertriglyceridemia (TG > 400 md/dl)
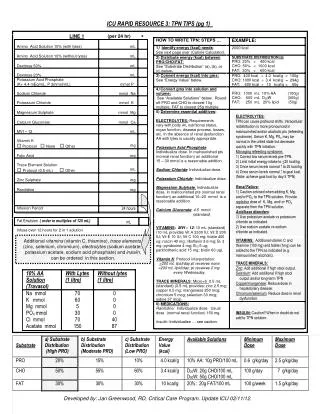
Components of TPN • Carbohydrate, Amino acid, Fat, Electrolyte, Water, Vitamin, Trace element • Standard solution • Dextrose, Amino acid • Electrolyte (Na, K, Cl, Mg, Ca, P) • Vitamin (A, B1, B2, Niacin, B6, Panthothenic acid, C, D, E, Zn, Cu, Mn, Cr) • Lipid emulsion
Dextrose-content Solution • 1 g glucose = 3.4 Kcal • 1 g glucose = 5 mOsm/L
TPN formula • B: standard solution • D: 8% A.A., high BCAA, low AAA; for hepatic disease • E: 35% Dextrose, 12% A.A.; for HD and water restriction • F: 29% Dextrose, 12% & 7% A.A.; for ARF with HD • G: 29% Dextrose, 7% A.A.; for ESRD
Mechanical complication • Insertion-of-catheter related: • pneumothorax, brachial plexus injury, subclavian and carotid artery puncture, hemothorax, thoracic duct injury and chylothorax, cardiac perforation, catheter malposition • Air embolism • Catheter fragment embolism
Metabolic complication • Fluid overload / Dehydration from osmotic diuresis • Hypertriglyceridemia • Hypocalcemia • Hypomagnesemia • Hypophosphatemia • Hyperglycemia / Rebound hypoglycemia on sudden cessation of TPN • Hyperammonemia • Hyperchloremic metabolic acidosis • NKHS
Infectious complication • Catheter-related sepsis: Staph. epidermidis and aureus; solution contamination • GNB for immunocompromise • Direct evidence: tip culture or blood culture • Indirect evidence: fever (up to 38C, 2 times, every 4 hours), chills, abrupt increase of blood sugar, hypotension, tachycardia, leukocytosis
Hepatic complication • Biochemical: elevated serum aminotransferase and alkaline phosphatase • Histological: steatosis, steatohepatitis, cholestasis, fibrosis and cirrhosis • Usually benign and transient, but severe in TPN for > 16 weeks • Additive use of Choline, Glutamine and Carnitine may be helpful • If cholestasis is present, Cu and Mg should be deleted to prevent acculumation in liver and BG
Biliary complication • Acalculous cholecystitis, GB sludge, cholelithiasis in TPN for > 3 weeks • Decrease of bile salt reabsorption leads to formation of GB stone; • Encouraging enteral intake to stimulate GB contraction
Intestinal complication • Villous atrophy: decreases in gut weight and mucosal height
Metabolic bone disease • Present in TPN for > 3 months • Bone pain, bone fracture or asymptomatic but demineralization in CxR • Possible mechanisms • Aluminum toxicity • Vitamin D toxicity • Negative calcium balance
Refeeding syndrome • The metabolic and physiologic consequences of the depletion, repletion, compartmental shifts and interrelationships of the followings • Phosphorus (< 1mg/dl, death within hours) • Potassium • Magnesium • Glucose metabolism • Vitamin deficiency • Fluid resuscitation
Case History • 66 y/o female, abdominal pain and anorexia for 6 weeks • persistent profuse, yellow, watery diarrhea after construction an ileal conduit for ureteral obstruction lasting for 3 months • PE: BW 36 kg, 70% of IBW; afebrile, 108, 14, 98/70 • anasarca, cachectic with generalized muscle wastage
Hct 38%, WBC 17000, BUN/Cr 22/1.0, K 3.4, P 3.4, HCO3 17, Sugar 48, Alb. 1.59 • Hospital Course • TPN was started with 750g dextrose, 120g AA, 60 mEq Na, 20 mEq K, 15 mmol P in 3L fluid • 24 hrs after start of TPN, HR 180, SBP 50, CVP < 3 cmH2O • P 0.7, Na 142, K 1.4, HCO3 19, Mg 1.8, • Sugar 1010, BUN/Cr 27/1.3 • pH 7.31, O2 59, CO2 24 (O2 2L)
Apnea and respiratory failure developed within one hour • With stopping TPN and fluid replacement, P 6.9, K 3.5 and Sugar 45 were obtained. • In the following hospitalization, bilateral pneumonia and ARDS were complicated. • Died on the 6th day • Autopsy: ischemic enterocolitis, pneumonia, ARDS and peritonitis and the heart was unremarkable
Sequence of events Within 48 hrs of starting TPN After correction of hypophosphatemia P, Sugar, K, Meta. acidosis GI bleeding, Sepsis Tachycardia, Hypotension Persistent Cardiopulmonary Instability Apnea, MV support Death ARDS, Pneumonia
Physiology of Starvation • When BMR = energy output to the limited intake, endogenous fuels must be used • Major storage fuel is fat in form of TG (60-75 days) • Carbohydrate, in contrast, is quantitatively insignificant storage fuel (1200 kcal, 1 day’s resting ER) • Protein, 12kg, 2 weeks’ worth of calories; but is for nonfuel function
Metabolic Response to Refeeding • A shift from body fat to CHO as major fuel source • Insulin • Glycogenolysis, gluconeogenesis and FA mobilization from adipose tissue is inhibited • Cellular uptake of glucose, K, P, and Mg is enhanced by insulin • Antinatriuretic effect (Na retention and ECF expansion)
Patient of risk for refeeding syndrome • Chronic alcoholism • Anorexia nervosa • Classic marasmus • Classic kwashiorkor • Chronic undernourishment • Morbid obesity with massive weight loss • Prolonged hypocaloric intravenous hydration • NPO for greater than 7-10 days • Cardiac and cancer cachexia
Be aware of the syndrome Recognize the patient at risk Correct electrolyte imbalance before initiating nutritional support whether by the oral , enteral or parenteral route Judiciously restore circulatory volume, monitor HR, and I/O Increase caloric delivery slowly Administer vitamins routinely Closely monitor electrolyte over the 1st week: Serum P, K, Mg, Sugar and urine electrolytes A little nutrition support is good, too much is lethal Recommendations to avoid refeeding syndrome