Download
1 / 45
600 likes | 1.33k Views
Laser of hair removal. by: DR Neda Adibi Dermatologist. WHAT IS HIRSUTISM?. The growth of unwanted and terminal hairs in androgen dependent area in the females called hirsutism The etiology is either idiopathic or due to androgen excess.

E N D
Laser of hair removal by: DR Neda Adibi Dermatologist
WHAT IS HIRSUTISM? The growth of unwanted and terminal hairs in androgen dependent area in the females called hirsutism The etiology is either idiopathic or due to androgen excess
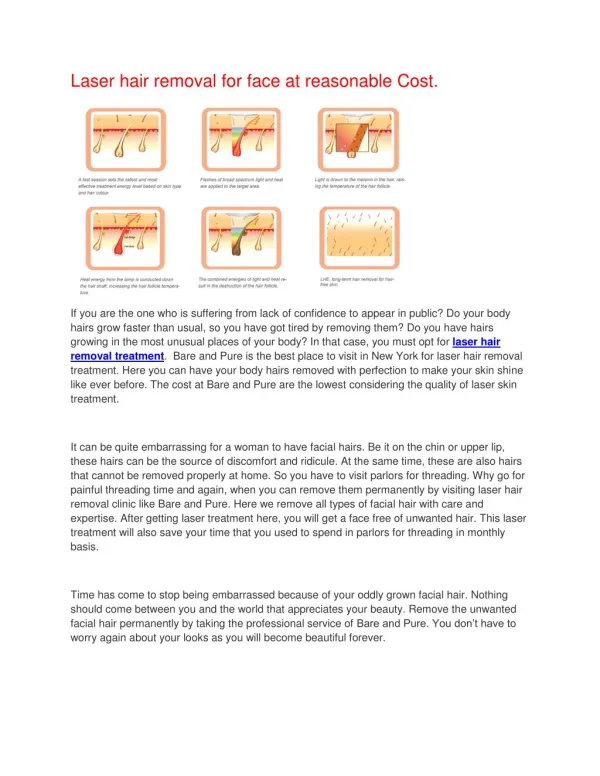
Hair follicle destruction by light source: (1) The damage may result from direct photothermal destruction, whereby a light source emitting a wavelength in the absorption spectrum of the desired chromophore melanin (600–1100 nm) results in selective heating of the hair shaft, follicular epithelium, and hair matrix..
Laser Hair Removal – How it works • The laser emits a gentle beam of light which is absorbed only by the hair follicle (leaving the skin unharmed). This light energy is transformed to heat which destroys the hair follicle permanently. That’s really all there is to it. • This is called ‘Selective Photothermolysis’.
Laser Hair Removal – How it works • The laser emits a gentle beam of light which is absorbed only by the hair follicle (leaving the skin unharmed). This light energy is transformed to heat which destroys the hair follicle permanently. That’s really all there is to it. • This is called ‘Selective Photothermolysis’.
Anagen follicles of terminal hair extend deeply into the subcutaneous fat, lying 2–7 mm below the skin surface.
The bulb of a telogen, or club, hair is unpigmented because of the cessation of melanin production during the catagen stage. In fact, the cessationof melanin production is the first sign of catagen. As anagen progresses, the bulb and papilla descend deeply into the dermis so that late anagen hairs may also be somewhat laser resistant to treatment. It would seem
, therefore, that it is in early anagen that hair follicles are most sensitive to laser induced injury. Since any injury, even a laser injury, may induce telogen, the timing of a second laser treatment after the first laser induced telogen formation, becomes critical. As the laser resistant terminal follicles now enter an anagen growth phase, after a first treatment, the second treatment may be more effective than the first. Conversely, a second treatment given too early, or too late, would be expected to have little effect.
Lin et al postulate that follicles treated in the telogen phase show only a growth delay for weeks, whereas, when those follicles are treated in the anagen phase they may be susceptible to lethal damage, may have a growth delay, or may simply switch into telogen phase. This could partly explain the growth dynamics of the hair cycle. Repeated treatments could lead to a synchronization of the anagen phase by induction and/or shortening of the telogenphase,which could increase the effivenessof hair removal with
Laser dermatology by GOLDBERG: Another explanation might be that the follicle is not destroyed immediately, but shows a growth arrest after only one (shortened) anagen cycle. Some have questioned the assumption that effective laser hair removal is determined solely by treating hairs in the anagen cycle. These investigators suggest that melanin within a hair follicle may be moreimportant than the actual time of treatment.
What is the definition of permanent hair loss? Permanence, defined as an absolute lack of hair in a treated area for the lifetime of the patient, may be an unrealistic goal. Dierickxet al. have suggested a more practical approach. They defined ‘permanent’ hair loss as a significant reduction in the number of terminal hairs, after a given treatment, that is stable for a period longer than the complete growth cycle of hair follicles at any given body sit
FDA definition: Permanent hair reduction is defined by the FDA as stable decrease in the number of terminal hairs for a period longer than the complete hair cycle at a given site following a treatment regime, which may include multiple sessions.
Why permanent hair removal is not possible? 1.Laser induces catagenphase 2.One of the uncertainties in laser hair removal is the exact tissue target. it appears that complete destruction of hair follicle without regeneration potential may occur when both the germinative cells in the bulb and the stem cells in the bulge area are destroyed. As follicular stem cells appear to be very resilient to thermal damage, this may be diffi cult to achieve
What is the role of anatomic siteon the outcome? It should be noted that there is a general consensus that hair removal results will always be affected by chosen anatomic site. Most investigators note a better response on chest, face, legs, and axilla. Lesser responses appear to occur on the back, upper lip, and scalp. In addition, terminal hairs, and not vellushairs respond to laser treatment. The ideal patient has realistic expectations, normal endocrine status, with thick dark hair and light skin tones .
There are differences in the anagen:telogen ratio depending on the area that is treated. For example the axillae and bikini areas have a higher anagen: telogenratio than the legs, arms, and chest. Therefore, it has been suggested that these areas would respond better to laser hair removal with more noticeable difference .in hair density
The role of parameters? It is now widely accepted that almost any laser can induce temporary hair loss. Fluences as low as 5 J/cm 2 can induce this effect. The effect tends to last 1–3 months. The mechanism of action appears to be an induction of catagen and telogen. Permanent hair reduction, occurring at higher fluences is seen in 80% of individuals and is fluence dependent. Thus, the greater the delivered fluence, all else being equal, the better are the expected results.
Dark hair with ample amounts of eumelanincan be effectively treated by multiple devices, provided that appropriate fluence and spot size are used. Under these conditions, the average long term hair loss per treatment is about 20-30% based on studies performed with ruby lasers. Multiple treatment sessions are usually required to achieve the maximal level of hair reduction. In individuals with blonde, red, gray, or white hair, it is unlikely that laser treatment will produce the same degree of longlasting hair removal. However, such patients may be willing to undergo treatments spaced about 2-4 months apart as necessary to maintain temporary hair loss.
While treatment can be safely performed with a shorter wavelength device (e.g. ruby laser) in fair skinned patients, it is preferable to use longer wavelength devices in darker skinned patients.
RUBY The first laser hair removal system employed was the normal- mode ruby laser, but the pulse duration of 0.3 ms was not efficacious longer pulse durations of 0.7-0.8 ms subsequently increased its usefulness. When the pulse duration of the ruby laser was lengthened to 3 ms, permanent hair removal was demonstrated however, there was a significant risk of dyspigmentation. In general, use of the ruby laser for hair removal is limited to patients with skin types I-III, since absorption of 694 nm light by epidermal melanin results in a higher risk of compli- cations (e.g. blistering, pigmentary changes) in individuals with darkly pigmented skin.
ALEXANDRATE BOLOGNIA: Multiple studies have demonstrated effective hair removal with the long-pulsed alexandrite laser at fluences of 10-40 J/cm2 and pulse durations of 2-20 ms. At fluences of 20-40 Jlcm2, several investigators have reported hair reductions of 70-80% after multiple (at least 3-5) treatments. Use of the long-pulsed alexandrite in patients with darkly pigmented skin has been reported, but side effects such as blistering and pigmentary alteration can occure in general, this laser is best suited for hair removal in patients with skin types I-III.
Red hair contains pheomelanin, which absorbs poorly at any wave-length, but especially beyond 800 nm. Therefore, shorter wave-lengths, such as those of ruby or alexandrite lasers are needed in these patients.
Which laser is suitable for individuals with low contrast between hair and skin? In cases of low contrast between skin tone and hair color, such as darkly pigmented individuals or light hair in fair individuals, a significant portion of emitted light is absorbed by the epidermal melanin. This occurs because epidermal melanin absorbs energy not only from direct exposure, but also from backscattering. As wavelengths of light increase, a greater ratio of dermal-to-epidermal deposition of energy results in greater safety in such individuals.
Diod:Both800 and 810 nm wavelengths are absorbed by melanin to a slightly lesser degree compared to the alexandrite laser. Absorption is also approximately 30% less than that of the 694 nm wavelength. Decreased absorption by epidermal melanin permits safe treatment in patients with skin types I to IV .
Although the rates of melanin absorption by diod laser is lower than the ruby and alexandrate, the rates of hair reduction with the diode laser are similar to those observed with the alexandrite laser, likely due to deeper penetration into the dermis . Treatment with the diode laser can be somewhat more painful, however, at least partly due to greater volumetric heating of tissue. If necessary, pain can be partially alleviated by reducing the frequency of delivered pulses.
A diode laser was safely used in several patients undergoing isotretinoin therapy without increase in adverse effect or longtermsequela,theisotretinoin use should be avoided in general up to 6 month beforehair removal.
Technique Laser treatments for hair removal are generally well tolerated by patients and do not usually require anesthesia. However, because the hair follicle is surrounded by nerve endings, topical anesthesia is necessary when treating large surfaces of the body or sensitive areas such as the upper lip and bikini area. Local infiltration of anesthetic or nerve blocks using 2% lidocaine can also be useful in selected patients.
Pulses are delivered in a slightly overlappingmode with a predetermined spot size. The ideal immediate response is vaporization of the hair shaft, followed erythema a few minutes later by the appearance of perifollicular edema and fluence and theIt is generally recommended that the highest tolerable largest spot size be used in order to obtain the best results. Larger spot size may accelerate the response , excessive fluences that cause epidermal separation or blistering should be avoided. If the device is not equipped with a cooling mechanism, a thick layer of cool gel is applied before the delivery of laser pulses.
Epidermal cooling during treatment accomplishes two goals. First, it minimizes the risk of epidermal damage due to absorption by epidermal melanin. Such damage may result in blistering, discoloration, and scarring, and is especially important for darker pigmented individuals. Therefore, epidermal cooling allows for use of higher fl uences while minimizing the risk of epidermal damage. Second, it has temporary anesthetic effect, thus reducing patient discomfort during treatment. Epidermal cooling can be separated into contact and non-contact. Contact cooling may include cold gel, chilled sapphire window, and cooled copper plate. Non-contact cooling includes cold air convection and dynamic cooling with automatic spraying of liquid cryogen, tetrafluoroethane, immediately prior to laser pulse.
After being scattered, photons closer to the center of the beam may, in fact, regain the initial direction of travel through their interaction with other photons. On the other hand, if scattered, photons at the periphery of laser beam may not be able to regain it. Therefore, the percentage of light lost to scattering is larger for smaller beam diameter, or spot size, than for a larger one. Two corollaries of this principle are that energy density, or fl uence, is lowered for larger spot sizes and that a very small spot size may, in fact, not allow for sufficient depth of penetration, even with longer wavelengths. Thus, the largest spot size accommodated by the size of the treatment area may lead to better efficacy, as well as decreased overall treatment time.
, the choice of fluencedepends on the amount of chromophoein the target structure, as well as selected wavelength.Higher fl uences are needed when the amount of chromophore is reduced, as represented by blonde or thinner-caliber hair. As well, as was previously discussed, higher fluencesare used with longer wavelengths due to the nearly linearly decreasing absorption of light by melanin at those wavelengths. In addition, fl uences diminish rapidly as a function of the depth of penetration, as progressive absorption and scattering result in decay of the original energy. Therefore, even though temporary hair removal will occur at almost any fluence, higher fluences may result in longer-lasting or more permanent hair reduction.
For all laser and light systems, the immediate treatment endpoint is vaporization of the hair shaft. This is followed in a few seconds to minutes by mild erythema and perifollicular edema. In general, these should resolve within 10 to 60 minutes. More widespread erythema or confluentedema may indicate epidermal and dermal damage, respectively. If noted, lower fluence, longer pulse duration, or better cooling should be utilized. Gray or white discoloration immediately following laser pulse and lasting a few seconds is an indication of epidermal damage and should be avoided.
Research has shown that laser hair removal requires the presence of a pigmented hair shaft. Retreatment can therefore be performed as soon as regrowth appears. Regrowth is based on the natural cycle, which varies by anatomic location , but on average, the timing is 6–8 weeks. More research regarding this is currently being conducted.
Repeated treatments may synchronize the anagenphase by induction and/or shortening of the telogen phase which could lead to increased effectiveness of hair removal at each consecutive treatment. Alternatively, the follicle may show growth arrest after one shortened anagen cycle
Temporary hair loss (1–3 months) always occurs after laser treatment, regardless of hair color or device used. On the other hand, the ability to induce long-lasting hair reduction is strongly correlated with hair color. Patients with dark hair are most likely to obtain longlasting hair removal. Blonde-, red-, gray-, or white-haired patients are unlikely to experience a permanent reduction, because melanin is low or lacking in the hair follicles.