Download

1 / 67
720 likes | 809 Views
Explore the epidemiology of Clostridium difficile infection, guidelines on who and when to test, testing methods, infection control measures, asymptomatic carriage, and the role of antibiotic stewardship. Learn about the impact of PPIs and probiotics, recurrence rates, virulence factors, and treatment strategies for this gram-positive bacterium causing severe diarrhea. With increasing incidence in healthcare and community settings, prevention strategies are crucial. Stay informed to combat this life-threatening infection effectively.

E N D
Clostridium difficile Dan Young
Objectives -Epidemiology -Who/When to TEST -HOW to test -Do you repeat testing (Spoiler alert: no) -Some infection control -Asymptomatic Carriage -Antibiotic Stewardship -PPIs? -Probiotics? -biomarkers? -Treatment
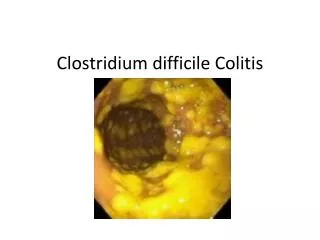
Intro Clostridium difficile is a gram positive, anaerobic, spore forming bacterium that causes invasive diarrhea ranging in severity from mild to life-threatening (1) C.diff was responsible for almost 500,000 infections, and 29,000 deaths in 2011 (2) 65 or older, white, females higher incidence 345,000 cases occurred outside hospitals (3), and 46% of cases were community associated (no documented healthcare exposure)
Intro Identified as the causative pathogen in the majority of cases of antibiotic-associated colitis in the 70s First described in 1935, named “difficult clostridium” because of difficulty related to isolation and growth on conventional media Can exist in spore form or vegetative form Spore form outside the colon- resistant to heat, acid, and antibiotics Convert to vegetative form inside the intestine. Fully functional form, which produces toxins and becomes susceptible to killing Two potent exotoxins: A and B, that mediate colitis and diarrhea Not an invasive organism. Non-toxinogenic strains don’t cause CDI Toxins inter the cells and inactive regulatory pathways, leading to ulceration of the intestinal mucosa (76, 77, 78, 79, 80, 81, 82)
Intro Toxin A (enterotoxin) causes inflammation that leads to intestinal fluid secretion and mucosal injury. Toxin B (cytotoxin) is essential for the virulence of C.diff and is over 10X more potent than toxin A 10-30% of strains don’t make toxin, and are not pathogenic
Intro Recurrence rates for healthcare-associated C.diff infection average 20% Can cause severe disease and death, mostly among healthcare-associated infection 9.3% fatality for HC-associated infection Most common strains: NAP1, NAP4, NAP11
Important Points C.diff no longer restricted to acute care settings High recurrence rate No vaccine We use too many antibiotics Prevention is a US priority with established targets by 2020 (5,6)
Epidemiology In the US, hospitalizations for C.diff infection doubled from 2000-2010 (3) C.diff infection is the leading cause of gastroenteritis-associated death, and the most common cause of healthcare-associated infection in US hospitals(7) Cost of C.diff infection is 4.8 billion for acute care facilities. (4) C.diff increasingly reported in the community and nursing home settings
Epidemiology Highest incidence in people over 65, female, white 65% health care associated, 37% hospital acquired 36% had onset in long term care facilities 28% were community onset, but most of those had outpatient healthcare exposure, so most of all CDI cases (94%) had some type of recent healthcare exposure(2) CDI surpassed MRSA as the most common cause of hospital acquired infection in a network of hospitals in the Southeastern US (8)
Epidemiology Severity has increased as incidence has increased: defined based on labs, exam, colectomy rates, ICU stay Emergence of PCR ribotype 027 epidemic strain (aka North American pulsed field type 1 [NAP1], or restriction endonuclease analysis pattern “BI” back in the 2000s in N America and parts of Europe (9)(10) After first diagnosis of CDI, 10-30% have at least one recurrent episode, and risk of recurrence increases with each successive recurrence (11)(12)(13)
Epidemiology $3427 - $9960 per episode $1.2 - $5.9 billion total US cost (14)
Epidemiology CDI in the community(15-18) Sources and risk factors are not well defined Most had some type of healthcare exposure 36% had no antibiotic exposure (12 weeks) 31% received PPI IBD (especially UC) at higher risk for primary and recurrent CDI CKD, ESRD Stem cell transplant recipients.
Colonization/Infection Transmission likely person to person through fecal-oral route or direct exposure to the contaminated environment (7) Asymptomatic colonization among adult inpatients 3%-26%, and <2% among asymptomatic adults without recent healthcare facility exposure Colonization rate upon hospital admission over 8%, with main risk factor being previous hospitalization (not antibiotic use or previous CDI) (19-24) “Incubation period” median 2-3 days (initial colonization to occurrence of disease (7,25,26)
Transmission Hands of healthcare personnel (C.diff spores) and environmental contamination are the main means of spread within healthcare (27,7) 3rd/4th gen cephalosporins, FQ , Carbapenem, clinda are high risk (28) Any antibiotic- suppression of normal gut microbiota. This is long lasting. Risk of C.diff increases during treatment and 3 months after cessation of therapy. Highest risk being during and in the 1st month following atb exposure (7,28) Longer exposure (time) and multiple antibiotics increase risk, but even a single dose increases risk
Other Risk Factors Cancer chemo- antibiotic activity of several chemo agents plus immune suppression HIV-because of immune suppression? Antibiotics or healthcare exposure? Both? GI surgery Advancing age PPIs (any breach in the protective effect of stomach acid) <--controversial. Several studies suggest an association but not clear IBD Low vitamin D (29-44)
Case 1 55 y/o lady admitted with AMI, developed diarrhea. She was placed on laxatives as needed on admission. C.diff test was ordered and came back positive. She had no abdominal pain, fever, or leukocytosis, and had not received any antibiotics
Diagnosis “Patients with unexplained and new-onset 3 or more unformed stools in 24 hours are the preferred target population for testing for CDI (weak recommendation, very low quality of evidence)” - 2018 Guidelines
Diagnosis If a patient has diarrhea symptoms not clearly explained by something else (IBD, tube feeds, chemo, laxatives, etc) testing for CDI is indicated However, some of those conditions are associated with increased risk for CDI We can optimize lab testing by only testing patients likely to have C.diff disease Don’t routinely test if laxative within the past 48 hours Labs can reject samples that are not liquid or soft Screening process
Diagnosis Testing - 2 approaches 1) Use a multistep algorithm (GHD plus toxin, arbitrated by NAAT, or NAAT plus toxin), instead of NAAT alone 2) Use a NAA alone or a multistep algorithm rather than toxin test alone when there are preagreed institutional criteria for patient stool submission
Diagnosis Testing options: all either detect either the organism or one or both of its major toxins (A and B) directly in the stool Toxigenic culture- grow it (reference method). Days Enzyme immunoassay (EIA) for toxin A and B detection. ‘80s and ‘90s- monoclonal or polyclonal Abs- overall poor performance Glutamate dehydrogenase (GDH)- detect the highly conserved enzyme present in high levels on All C.diff isolates (tox and non tox strains). Non specific, so combine with another test like EIA Nucleic acid amplification tests (NAATs)- gene targets. sensitive
Real quick, what is NAA? Detects genetic material rather than antigen or antibody Early diagnosis of a disease because detection of antigen requires antigen to appear in the bloodstream Genetic material is small NAT uses an amplification step (done by PCR, or other ways) This uses DNA or RNA base pairing- single stranded probe or primer molecules capture DNA or RNA target molecules of complementary strands NAATs target and amplify conserved nucleic acid sequences that are always present in strains of whatever you are looking for Very sensitive
Diagnosis Best way to test? “Remains elusive” ←-smart guys that wrote the guidelines Recommendations are strong, but low quality of evidence If Labs have no screening criteria and accept all unformed stools for testing, they recommend a multstep algorithm, like GDH/toxin plus NAA as a “tiebreaker”. OR NAAT or GDH followed by a high-performing toxin assay
Back to Case 1 55 y/o lady admitted with AMI, developed diarrhea. She was placed on laxatives as needed on admission. She had no abdominal pain, fever, or leukocytosis, and had not received any antibiotics NAAT- positive Toxin - negative She is a “carrier” NAAT- positive Toxin- positive True CDI
Diagnosis Option 2 Use NAA alone or a multistep algorithm for testing rather than a toxin test alone when there are preagreed institutional criteria for patient stool submission
Diagnosis Interview patients to see if they meet criteria for C.diff testing PCR is very sensitive and outperforms other diagnostic tests when applied to patients who meet clinical criteria for C.diff disease. Summary: careful screening (3 or more loose stools in 24 hours or less, with history of antibiotic exposure). Test those for CDI, using a highly sensitive test like NAAT alone, or in a multistep algorithm. 2 or 3 stage approach is probably better than one stage.
Diagnosis Don’t retest within 7 days (in the absence of any changes or new supporting clinical evidence) Multiple tests were done when we used tests with low sensitivity diagnostic yield is 2% (45, 46) Highly sensitive testing strategies have a very hight negative predictive value for CDI (7) Don’t test asymptomatic patients unless you are writing a paper In an asymptomatic patient with high clinical suspicion of CDI but negative test, expecially worsening, repeat testing should be considered. But just don’t ROUTINELY retest Recurrence of C.diff is common. So recurrent symptoms after successful treatment and resolution of diarrhea should be retested.
Huh? Just pick a strategy and go with it. We don’t know the best way to do it (obviously) Use your brain
Real Life Local hospital in NWA, screening by nurses On admit, isolate and do C.diff NAAT if: Current unexplained diarrhea Atb use within the past 4 weeks Diarrhea and fever or leukocytosis or abdominal pain During hospital stay, isolate and do C.diff NAAT if: Liquid or loose stool (at least 3 in 24 hours) Not on tube feeds
Real Life VA Before ordering a C.diff test Laxative? Other meds? Another organism? Another disease? Lab won’t run repeat tests within 7 days Diarrhea? At least 3 stools in 24 hours Discourage empiric tx (they get the test back 2-4 hours) Results- 130 orders/month to around 50-60/month
Best Approach Screen the patients (I like the approach done locally) If positive, then screen (wait, didn’t we just screen?) with NAAT or GDH, followed by High performance toxin test I think? Maybe Weak recommendation, low quality of evidence And don’t test for cure. Over 60% of patients remain C.diff positive even after successful treatment (7, 47, 48)
Other Biomarkers Fecal lactoferrin Calprotectin Cytokines IL8, IL1 beta, and other $h&t No
Infection Control (Some, mind you) Private room Decrease transmission to other patients Gloves and gowns All healthcare personnel On entry to a room Isolation measures Preemptive contact precautions pending test result if test results can’t be obtained the same day Continue for at least 48 hours after resolution of diarrhea C.diff undetectable in stool by time of reslution of diarrhea (48) But skin/environmental contamination is high
Infection Control (Some, mind you) Hand hygiene (assumes glove use) Transmission commonly occurs via hands of HCWs C.diff spores are resistant to killing by alcohol But studies have not shown an association between use of alcohol based products and increased risk of CDI After implementation of alcohol based products, MRSA and VRE rates dropped, but C.diff remained the same Guidelines punt, and finally recommend “to preferentially use soap and water
Infection Control (Some, mind you) Should we screen for asymptomatic carriage and isolate them? No Data, so in other words no
Stewardship What is the role of Antibiotic Stewardship? Get a program Requires “money” Reduce antibiotics Formulary restrictions Prospective audit and feedback Reduce FQ, cephalosporins, lincomycins, macrolides, PCNs, tetras, monobactams, sulfonamides, glycopeptides, aminoglycosides, carbapenems, oxazolidinones, glycopeptides, and inhaled tobramycin
Stewardship Number and duration of antibiotics Incidence might increase with number of abx given Cumulative antibiotic exposure Also, large study in Lancet ID 2017: ASP reduces incidence of: MDR GNs by 51% ESBL producers by 48% C.diff by 32% Improved patient outcomes Reduce adverse events Improve antibiotic susceptibility Optimize resource utilisation (money)
PPIs Epidemiologic association with PPI use and CDI(7, 49) Despite studies showing increased risk, practical application is limited (7) Appears to be a clinical association between PPI and CDI but the relationship is unclear (7) “A recommendation to globally discontinue PPI in patients at high risk for CDI or recurrent CDI regardless of need for PPI will require further causal proof” (7) “However, stewardship activities to discontinue unneeded PPIs are warranted” (7)
Probiotics $30-40 billion USD $57.4 billion USD by 2022 In 2012, use in the US was 4x higher than in 2007 1.6% of U.S. adults used Some are expensive ($120 lotion) No role in prevention for CDI (or anything else) In fact, we don’t really know if they do anything at all But it has 11 different strains! Mine has 61 billion colonies per serving! Sorry My recommendation: Brew beer. Make sauerkraut
Ancillary Strategies If CDI suspected Stop antitiotics asap. Continued use associated with decreased clinical response and increased risk of recurrence (7,50) Start treatment ONLY if there will be a delay in diagnosis, or you suspect fulminant CDI (7)
Treatment Initial treatment No difference between outcomes with vanco and metro in the 80s and 90s, small studies Later RTCs have shown vanco to be superior Later showed metro inferior to oral vanco for cure and 21-20 day recurrence after treatment (51, 52, 53, 54, 55)
Treatment 10 days tx used in almost all RCTs Some have a delayed response and are not resolved by day 10, especially on metronidazole Consider 14 days if not resolved by 10 Oral metro should be used only in non severe CDI when other treatments are not available or contraindicated Limit to one course of metro, due to potential neurotoxicity Peripheral neuropathy Dizziness Vertigo Headache Cerebellar toxicity (rare but serious)
Treatment 10 days tx used in almost all RCTs Some have a delayed response and are not resolved by day 10, especially on metronidazole Consider 14 days if not resolved by 10 Oral metro should be used only in non severe CDI when other treatments are not available or contraindicated Limit to one course of metro, due to potential neurotoxicity Peripheral neuropathy Dizziness Vertigo Headache Cerebellar toxicity (rare but serious)
Treatment Factors that correlate with more severe disease and treatment failure Fever (>38.5C) WBC >15K creatinine >1.5mg/dL Age Treatment with systemic antibiotics Underlying malignancy Renal insufficiency The guidelines use WBC and creatinine to help distinguish between non-severe and severe CDI
Treatment Vancomycin vs fidaxomicin Two RTCs (56,57) Fidaxo vs Vanco for CDI, NEJM 2011 F vs V for 10 days 629 patients Primary endpoint: cure Secondary: recurrence of CDI within 4 weeks, and “global cure” (cure with no recurrence) Fidaxo non inferior to vanco, and associated with a significantly lower rate of recurrence of CDI associated with non NAP1 strains
Treatment Vancomycin vs fidaxomicin Two RTCs (56,57) F vs V for infection with C.diff in Europe, Canada, and the USA: a double-blind, non-inferiority, randomised controlled trial (lancet ID 2012) 535 patients Fidaxo was NI to vanco Adverse events were the same Concluded fidaxomicin has similar safety and efficacy to vanco
Treatment Fidaxomicin First in class macrocyclic antibiotic A locally acting macrolide derived from fermentation of the actinomycete Dactylosporangium aurantiacum Active against C.diff (vanco is broad in the gut) Little activity for inhibiting other bowel flora spp Very high fecal concentrations Substantially higher inhibitory activity Bactericidal More prolonged post antibiotic effect (6-8 hours) Narrower in spectrum
Treatment Fidaxomicin Side effects Nausea 11% Vomiting 7% Abd pain 6% GI hemorrhage 4% Neutropenia 2% Anemia 2% Category B 200 BID X 10 days $100 a tab inpatient? $4000?
Treatment Vanco is a lot cheaper. Oral solution approved in 2018 Metro $20 Guidelines recommend considering fidaxomicin along with vanco as DOC for initial episode of CDI Other drugs (less evidence) Nitazoxainde Fusidic acid Rifaximin Tigecycline bacitracin
Treatment Recommendation Initial episode, non-severe (WBC <15K, Cr <1.5mg/dL Vanco 125mg PO 4x daily 10 days Fidaxomicin 200mg 2x daily 10 days They took metro out unless you don’t have anything else Initial episode, severe (>15, >1.5) Vanco, same Fidaxo, same