Download
1 / 47
470 likes | 635 Views
MICROSATILLITE INSTABILITY IN CRC HENRY T. LYNCH, MD JANE F. LYNCH, BSN Creighton University School of Medicine Omaha, Nebraska. Colorectal Cancer. Worldwide estimates for colorectal cancer during 2008*: Incidence – 1,233,711 Mortality – 608,644

E N D
MICROSATILLITE INSTABILITY IN CRC HENRY T. LYNCH, MD JANE F. LYNCH, BSN Creighton University School of Medicine Omaha, Nebraska
Colorectal Cancer • Worldwide estimates for colorectal cancer during 2008*: • Incidence – 1,233,711 • Mortality – 608,644 • Worldwide estimates for familial/hereditary CRC during 2008*: • Lynch syndrome 3-5% of all CRC 37,011-61,686 • FAP <1% of all CRC <12,337 • Familial 20% of all CRC 246,742 • *GLOBOCAN. The International Agency for Research • on Cancer web site. URL: http://www.iarc.fr/
Familial/Hereditary CRC in US Annual CRC incidence in US: 142,570 Lynch syndrome 3-5% of all CRC 4,277 - 7,129 FAP <1% of all CRC <1,426 Familial 20% of all CRC 28,514 Jemal et al. CA Cancer J Clin 60:277-300,2010. 3
Magnitude of the Problem • Question: Why are these figures of such significant public health impact? • Answer: Each hereditary cancer comes from a family that could benefit immensely from genetic counseling. • DNA testing, surveillance, and highly-targeted management are the key! • Problem: Significance of family frequently missed!
Should we test all colorectal cancer for Lynch Syndrome? YES! Test everybody.
Search for LS Among CRC Affecteds* Evidence: Among 500 CRC patients, 18 (3.6%) had LS. Of these 18: 18 (100%) had MSI-H CRCs; 17 (94%) were correctly predicted by IHC; only 8 (44%) were dx < 50 years; only 13 (72%) met the revised Bethesda guidelines; 1/35 cases of CRC show LS. *Hampel et al. J ClinOncol 26:5783-5788, 2008.
Molecular Genetic Screening for LS • Recommendation*: • All incident CRC and EC cases should be molecularly screened for LS. • MSI highly sensitive (89.3%). • IHC equally sensitive (91.2%), is inexpensive, is more readily available, and predicts the nonworking gene. • IHC is preferred method to screen for LS*. • *Hampel et al. J ClinOncol 26:5783-5788, 2008.
Familial CRC • Familial clustering of CRC, like that for carcinoma of the breast and stomach, has been discussed for more than 100 years. • What does it mean from the standpoint of risk? • Best answer – First- degree relative of CRC affected has 2-3 fold excess risk for CRC compared to population expectations.
Cardinal Features of Lynch Syndrome • • AD – MMR mutations • • Proximal • • Earlier age of onset • • Accelerated carcinogenesis • • Extra colonic cancers • • Pathology – distinctive? • • ↑ survival
Increased risk for certain extracolonic malignancies • Endometrial • Ovary • Stomach • Small bowel • Pancreas • Liver and biliary tree • Muir-Torre cutaneous features • Brain, (glioblastoma) – Turcot’s syndrome • Possible Prostate cancer and others • Breast cancer - controversial.
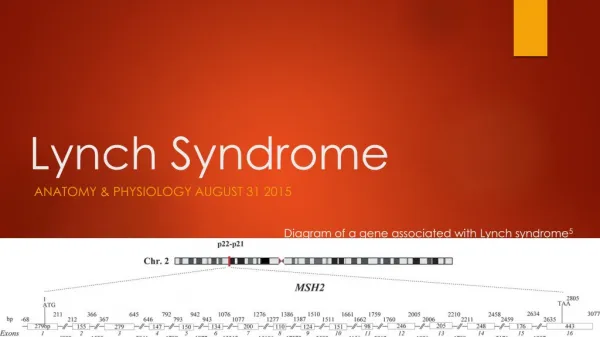
Cardinal Features of Lynch Syndrome • • Differentiating pathology features of LS CRCs: • - more often poorly differentiated; • - excess of mucoid and signet-cell features; • - Crohn’s-like reaction; • - medullary features; • - significant excess of infiltrating lymphocytes • within the tumor. • • Increased survival from CRC. • • Sine qua non for diagnosis is identification of germline mutation in MMR gene (most commonly MLH1, MSH2, MSH6) segregating in the family.
A B C D
Bethesda Guidelines and MSI Testing • MSI-H findings are associated with a moderate degree of uncertainty. • Such patients with MSI-H will merit referral for further genetic assessment. • Centers of expertise recommend informed consent for MSI testing.* • BRAF mutation, if present, will negate an LS diagnosis. • *Palomaki et al. Genet Med 11:42-65, 2009.
Cost-effectiveness of DNA Testing • Estimate of the cost-effectiveness of genetic testing strategies to identify LS among newly dx CRC patients using MSI and IHC is cost-effective.* • *Mvundura et al. Genet Med 12:93-104, 2010.
Amsterdam Criteria • AC-I (24) • At least three relatives with histologically verified • colorectal cancer; • One is a first-degree relative of the other two; • At least two successive generations affected; • At least one of the relatives with colorectal cancer diagnosed at <50 years of age; • Familial adenomatous polyposis (FAP) has been excluded.
Amsterdam Criteria ~60% of Amsterdam + Families have MSI-H and MMR mutations.
Familial CRC Type “X” • Amsterdam Criteria positive but lacking MSI and MMR mutations will constitute ~ 40% of those AC-I without MMR mutations and therein referred to as familial CRC type X.* • 1) CRC > left side • 2) CRC and extra colonic CRC • 3) Later age CRC onset • 4) Molecular genetics (MSI and IHC or MMR • mutation) ABSENT! • *Lindor et al. JAMA 293:1979-1985, 2005.
Epithelial Cell Adhesion Molecule (EPCAM) Gene and Its Lynch Syndrome Connection* • A portion of this ~40% lacking MMR mutations is caused by a mutation mechanism in the gene known as EPCAM. • *Kovacs et al. Hum Mutat 30:197-203, 2009.
5’ EPCAM deletion Exons 8 and 9 and polyadenylationsequence Polyadenylation Sequence Transcriptional read through Hypermethylation of the MSH2 promoter Ligtenberg MJ, Nature Genetics 2009.
Why LS with Site-Specific CRC? • Deletion in EPCAM results in hypermethylation and incomplete silencing of MSH2. • EPCAM mutation carriers may have phenotypic features that differ from carriers of MSH2 mutations – namely, an almost exclusive expression of site-specific CRC, thereby lacking extracolonic cancers.
American and Dutch families have the same deletion in the EPCAM gene MSH2 EPCAM Deletion c.859-1462_*1999del (4.9 kb, starting in intron 7 and including exons 8 & 9) Lightenberg, Nature Genetics 2009.
American and Dutch EPCAM mutations originate from a common ancestor Chromosome2 Chromosome 2 Dutch Families Family R Family R and the Dutch families share a 6.1 MB region surrounding the same EPCAM deletion indicating a common ancestor. Based on the size of the shared region it is estimated the deletion occurred 10 generations ago. Deletion and Region inherited from common ancestor
History of Family R* • Ascertained by us in 1970 and followed continuously. • 700 blood line relatives • 327 individuals age ≥ 18, ≥ 25% pedigree risk • Phenotype strikingly similar to LS but integral extracolonic cancers absent (site-specific CRCs) • *Lynch et al. Cancer 56:934-938, 1985. • Lynch et al. Cancer 56:939-951, 1985.
First patient identified with EPCAM mutation EPCAM results CRC affecteds
MSI in CRC* • Microsatellite instability (MSI): • a) is hypermutable phenotype due to loss of DNA • MMR activity; • b) is present in ~ 15% of all CRCs; • c) ~ 3% associated with LS, remaining 12% • sporadic acquired hypermethylation of promoter • of MLH1 gene; • d) occurs in tumors manifesting the CpG island • methylator phenotype. • * Boland and Goel. Gastroenterology 138:2073-2087, • 2010.
What Is MSI?* • Nearly all LS tumors differ from their sporadic counterparts and most are characterized by MSI. • MSI mutations occur at short repetitive sequences called microsatellites. Most are insertion or deletion mutations and, as a consequence of loss of DNA MMR activity. • *Boland & Goel. Gastroenterology 138:2073-2087, 2010.
Definitions of MSI’s Dx Criteria • These comprise BAT-25 and BAT-26 mononucleotides and D5S346, DS123, and D12S250 dinucleotide repeats. • > 2 or more markers → MSI-H; • those with one unstable marker MSI-L; • those absent instability referred to as MSS.
BRAFV600E Mutations in MSI* • The BRAFV600E mutation occurs exclusively in sporadic forms of MSI CRC. • Combined analysis of MSI and BRAFV600E mutation is included in current protocols of LS since it is a reliable, fast, and low-cost strategy. • Helps identify sporadic cases and avoids time-consuming and expensive screening of MMR germline mutation analysis. • *Seruca et al. Expert Rev Gastroenterol Hepatol 3:5-9, 2009.
Algorithm • IHC on all colorectal patients on tumor block; • If positive, BRAF (if positive, then sporadic); • Only do full MMR genetic tests on patient IHC +. BRAF neg.
MORPHOLOGY SUSPICIOUS FOR MSI-H Run PCR test for MSI status Is there MSI-H? FAMILIAL CRC TYPE “X” NO EVIDENCE OF LYNCH SYNDROME NO NO YES Is there loss of staining with any of the Abs? PUTATIVE LYNCH SYNDROME Run mutation analysis for BRAF V600E YES Is there BRAF V600E mutation? NO MMR GENES MUTATION ANALYSIS IHC for MLH1, MSH2, MSH6, PMS2 YES Is there a mutation in MMR gene? SPORADIC CRC WITH MSI-H NO YES LYNCH SYNDROME Gatalica Z, Torlakovic E. Fam Cancer 2008;7:15-26
MSI Analysis A functional assay for the MMR proteins
MSI High Data New – Focus on Mononcleotides
MSI and Therapeutic Implications • Pharmacogenetics: • 5-FU-based chemotherapy refractory in MSI CRCs; • possible advantage of irinotecan-based therapy; • the latter “not ready for prime time” but 5-FU approaching clinical acceptability. • Boland and Goel. Gastroenterology 138:2073-2087, 2010.
MSI and Therapeutic Implications* • Where did this knowledge originate? • Through DNA MMR genes first identified in bacteria through exposure to cytotoxic mutagens (alkylating agents) and selecting for strains resistant to DNA damage. • *Carethers et al. J Clin Invest 98:199-206, 1996. • Ribic et al. N Engl J Med 349:247-257, 2003.
MSI and Therapeutic Implications* • Resulting bacteria were hypermutable and resistant to DNA alkylation. • Resistant to cytotoxic agents that acted by damaging DNA. • Raised possibility that DNA MMR deficient cells might be relatively resistant to some types of cytotoxic chemotherapy. • *Carethers et al. J Clin Invest 98:199-206, 1996. • Ribic et al. N Engl J Med 349:247-257, 2003.
MSI and Therapeutic Implications • Virtually all studies show either no benefit or adverse effects in response to 5-FU-based adjuvant chemotherapy (reviewed by Boland and Goel.*) • In vitro responses suggest that chemoresistance is seen for many chemotherapeutic agents.** • *Gastroenterology 138:2073-2087, 2010. • **Aebi et al. Cancer Res 56:3087-3090, 1996.
MSI and Therapeutic Implications* • Currently, guidelines do not recommend using MSI status to determine whether or not to use chemotherapy. • This recommendation merits a second look, given the wealth of data showing the inadequacy of 5-FU for CRC with MSI. • Should be tested only in the context of a randomized clinical trial. • *Boland & Goel. Gastroenterology 138:2073-2087, 2010.
Immune Response in CRCs with MSI • CRCs with MSI demonstrate a host-immuneresponse characterized by tumor infiltrating lymphocytes (TILs): • may exert effects on tumor cell apoptosis and cell proliferation; • associated with improved disease-free survival; • *Sinicrope et al. Int J Cancer 120:1232-1238, 2007.
Immune Response in CRCs with MSI • (continued:) • Apoptosis/proliferation ratios and reduced cell proliferation; • Phenotypic features of MSI-H tumors, associated with ↑ TILs; • Indicate an activated immune response that may contribute to their favorable survival rates. • *Sinicrope et al. Int J Cancer 120:1232-1238, 2007.
Host Immune Response Characterized by Tumor Infiltrating Lymphocytes (TILs)* • Summary: • Higher apoptosis/proliferation ratios and reduced cell proliferation are phenotypic features of MSI-H tumors that are associated with ↑ TILs; • Indicating an activated immune response, and may contribute to their favorable survival rates. • *Sinicrope et al. Int J Cancer 120:1232-1238, 2007.
IHC and LS • IHC is an acceptable substitute for MSI, given strong concordance rates of 94% between MSI and IHC in CRC and EC.* • Allows gene-specific DNA analysis based on staining pattern. • MMR protein deficiency occurs in 12-20% of CRCs.** • *Palomaki et al. Genet Med 11:42-65, 2009. • **Hampel et al. J Natl Comp Cancer Net 8:597-601, 2010.
Targeted CRC Screening • Screening is melded to LS’s natural history: • Proximal location colonoscopy • Early age of onset beginning at age 25 • Accelerated carcinogenesis every 1-2 yrs < age 40,then annually • Pattern of extra-colonic cancers targeted screening
MSI/IHC in CRC* • Conclusion: • CRCs with MSI may show distinctive clinical, pathologic features: • a) predominance of CRC in proximal colon; • b) lymphocyte infiltration within tumor; • c) poorly differentiated mucinous or signet cell • appearance; • d) better prognosis; • e) differing response to chemotherapeutics; • f) molecular screening all CRC cases. • *Boland and Goel. Gastroenterology 138:2073-2087, 2010.