Download
1 / 71
740 likes | 939 Views
RIGHT ILIAC FOSSA MASS-DDS & INVESTIGATIONS. BY ZIYANA LIYAKATH 2002 BATCH. ILIAC FOSSA REGION-ANATOMYY. TOPOGRAPHY OF RIF. Swellings in RIF. PARIETAL rare except iliac abscess/appendicular abscess burrow through anterior abdominal wall & may become parietal INTRA ABDOMINAL Two types

E N D
RIGHT ILIAC FOSSA MASS-DDS & INVESTIGATIONS BY ZIYANA LIYAKATH 2002 BATCH
Swellings in RIF • PARIETAL • rare except iliac abscess/appendicular abscess burrow through anterior abdominal wall & may become parietal • INTRA ABDOMINAL • Two types • Structures normally present in the site • Structures abnormally invade region
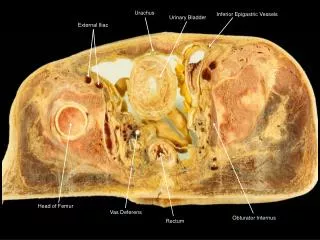
NORMALLY PRESENT • APPENDIX • CAECUM • TERMINAL PART OF ILEUM • LYMPH NODES • ILIAC ARTERIES • RETROPERITONEAL CONNECTIVE TISSUE Gross
ILIOPSOAS SHEATH • ILIUM
ABNORMALLY INVADE • RENAL SWELLING • GALL BLADDER SWELLING • UTERINE SWELLING • URINARY VESICAL • UNASCENDED TESTIS • PELVIC ABSCESS
ANATOMY • Average length:7.5-10 c.m • Position->retrocaecal(44%),pelvic(21%),subcaecal(1.5%),postileal(.5%),paracaecal(2%),preileal(1%) • Histology->mucosa,sub mucosa,muscularis propria,serosa • Mesentry->meso appendix • Blood supply->appendicular artery,acessory appendicular
APPENDICULAR MASS • Third day or earlier after attack of appendicitis • At the position of appendix • O/E->irregular firm tender & fixed mass • Rigidity of abdominal musculature • Tympanitic on percussion • CONSTITUENTS • Inflamed appendix • Greater omentum • Oedematous caecal wall • .coils of small intestine
APPENDICULAR ABSCESS • Failure of resolution of appendix mass • Continued spiking pyrexia
RARE • MUCOCELE • When proximal end of lumen slowly becomes completely occluded by fibrotic stricture & retained sterile secretions ,appendix enlarged greatly & sometimes contains several milli litres of mucus • When infection supervenes empyema develops
NEOPLASMS • CARCINOID TUMOUR[ARGENTAFFINOMA] • Arise from argentaffin tissue[kulchitsky cells of crypts of lieberkuhn],most commonly in vermiform appendix • 10 times more common • Frequently distal 3rd • Feels hard
CARCINOMA CAECUM • Patient above 40 • Hard fixed lump • May not be any change in bowl habit if present alternate constipation & diarrhoea • Anemia,anorexia,weight loss
AMOEBIC CAECAL MASS • Entamoeba Histolytica • Tenderness on deep palpation over caecum & sigmoid
ACTINOMYCOSIS • Hard & fixed mass • Multiple sinuses seen discharging sulphur granules • Discoloration of affected skin
TERMINAL ILEUM • IMPACTION OF ROUND WORMS • Lower part of ileum • History of passing worm with stools/vomitus
CROHN’S DISEASE • CLINICAL FEATURES • INFLAMATORY STAGE • Tender mass • Fever • Anemia • Diarrhoea • COLITIS STAGE
Diarrhoea,fever,anemia,loss of weight,occult blood & mucus present in stool • Steatorrhoea • Fissure in ano • Perianal abcess • Anal fistula • STENOTIC STAGE • Small intestinal obstruction
FISTULA • External/internal
ILEOCAECAL REGION • HYPERPLASTIC ILEOCAECAL TB • Injection of mycobacterium TB.Infection starts in lymphoid follicles &then spreads to submucous & subserous planes • Intestinal wall thickened,lumen narrowed • Matted lymphnodes+terminal part of ileum & caecum involvement produced lump
Gross specimen of ileum showing multiple hypertrophied tubercular pseudopolyps and cut part of appendix Gross specimen of ileum showing multiple hypertrophied tubercular pseudopolyps and cut part of appendix Gross specimen of ileum showing multiple hypertrophied tubercular pseudopolyps and cut part of appendix Gross specimen of ileum showing multiple hypertrophied tubercular pseudopolyps and cut part of appendix Gross specimen of ileum showing multiple hypertrophied tubercular pseudopolyps and cut part of appendix Gross specimen of ileum showing multiple hypertrophied tubercular pseudopolyps and cut part of appendix Gross specimen of ileum showing multiple hypertrophied tubercular pseudopolyps and cut part of appendix
COMPLAINTS • 1.Recurrent attacks of abdominal pain with diarrhoea • 2.Blind loop syndrome • 3.lump • 4.general
LYMPH NODES • Enlargment of iliac group of lymphnodes • A.FILARIAL • Periodic attacks of fever with simultaneous tenderness & swelling of nodes
B.TUBERCULOUS LYMPH NODE • GENERAL FEATURES • Matted lymph nodes
C.LYMPHOSARCOMA • Rapid enlargment of nodes • Young subject • D.SECONDARY CARCINOMA • Other evidence of primary ca • Usually old
ANEURYSM OF ILIAC ARTERIES • RARE
ILIOPSOAS SHEATH • ILIAC ABSCESS • Infection of haematoma in iliacus muscle • Pain,tenderness restricted to region • Clear space btw abscess&ilium
PSOAS ABSCESS • Down the thoracolumbar vertebra to pelvis&crosses inguinal ligament to thigh • Cross fluctuation present
ILIUM • Bony swelling
ABNORMALLY INVADING • 1.KIDNEY • A.PELVIC KIDNEY • The first rudiment appear in pelvis • With development ascend to final position • Due to unknown reasons kidney fail; to ascend & remains permanently in pelvis/right iliac fossa • B.DROPPED/MOVABLE KIDNEY • Extremely rare
GALL BLADDER SWELLING • Hugely distended gall bladder with enlarged liver descend as low as right iliac fossa
h/o vaginal discharge • Menstrual irregularities • p/v can confirm clinically • A.tubo-ovarian mass • B.pyosalpinx • C,.cyst & abscess of broad ligament • D.fibroid of uterus • E.ovarian cyst
UNDESCENDED TESTIS • Develops in lumbar region • As foetus grows,testis descends through inguinal canal into scrotum • Fails to descend • Commonest-superficial ing pouch
PELVIC ABSCESS • Most common presentation-spiking pyrexia • Pelvic pressure/discomfort associated with loose stool,tenesmus • P/R->Boggy tender mass in pelvis anterior to rectum
1.ROUTINE BLOOD • A.ANEMIA-malignancy,tuberculosis,crohn’s disease • B.ESR-malignancy,tuberculosis,crohn’s disease
C.POLYMORPHONUCLEAR LEUCOCYTOSIS • D.EOSINOPHILIA • E.MICROFILARIAE
2.URINE • UTI • RBCs • 3.STOOL • Occult blood • microscopy
4.TUBERCULOUS ETIOLOGY • Psoas abscess,ileocaecal T.B,lymphnode • AFB STAIN • C & S • LUMBAR X-RAY,DORSAL SPINE X-RAY