Download
1 / 16
160 likes | 264 Views
Data on Brain Injury in Massachusetts: A Snapshot . Jean McGuire Executive Office of Health and Human Services Presentation to the Brain Injury Commission February 7 th , 2011. Current Types of Data with State Specific Information on Brain Injury. Acute Care Hospital Discharge Databases

E N D
Data on Brain Injury in Massachusetts: A Snapshot Jean McGuire Executive Office of Health and Human Services Presentation to the Brain Injury Commission February 7th, 2011
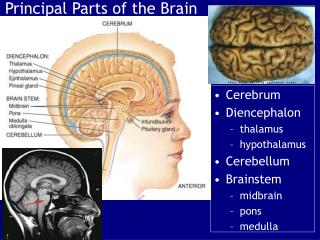
Current Types of Data with State Specific Information on Brain Injury • Acute Care Hospital Discharge Databases • Vital Statistics – Death File • Statewide Trauma Registry Data • Disease Specific Surveillance Data • Brain Injury Symptom Surveillance Data
Acute Care Hospital Discharge Databases • MA Emergency Department Discharge Database • MA Inpatient Hospital Discharge Database • MA Outpatient Observation Stay Database • This data is maintained by MA Division of Health Care Finance and Policy Strengths: • Contain discharge information on all cases discharged from any acute care hospital in Massachusetts • TBI-related cases are determined according to standardized case definitions recommended by the Centers for Disease Control and Prevention (CDC) and are based upon International Classification of Disease Version 9 Clinical Modification (ICD-9-CM) codes for morbidity and International Classification of Disease Version 9 (ICD-9, 1995-1998) and Version 10 (ICD-10, 1999-2006) codes for mortality Limitations: • These administrative databases contain information which is collected for billing purposes but which are used secondarily for surveillance. • Does not tell us prevalence of injury that results in long-term disability • Information has not been validated by medical record review
Emergency Department (ED) Discharges, Inpatient Hospital (HDD) Discharges, and Observation Stay (OBS) Discharges for All and TBI-related Injury Cases by Leading and Selected Causes of TBI, MA Residents, FY 2008
Vital Statistics – Death File • Registry of Vital Records and Statistics • Maintained by MA Department of Public Health • Summary statistics can be found in handout: Traumatic Brain Injuries in Massachusetts: Data Summary, September 2008. This report is prepared by MA DPH, Injury Surveillance Program
State Trauma Registry Data • Erwin Hirsh Statewide Trauma Registry • Maintained by MA Department of Public Health, Office of Emergency Medical Services • Captures physiologic information providing details on the severity of injury with clinical markers Challenges with data source: • Only captures cases which are hospitalized, requiring interfacility transfer, or cases resulting in death • Data currently being validated
Disease Specific Surveillance Data—Stroke Registry • The Paul Coverdell National Acute Stroke Registry (PCNASR) collects emergency department and inpatient data on patients arriving to hospitals • MA is one of 6 states with federal funding to maintain a PCNASR • In MA, approximately 85% of all stroke hospitalizations (11,000 a year) are captured in the registry • 58 MA hospitals are currently participating in the registry • This registry is maintained by MA Department of Public Health
Statistics from Stroke Registry • Strokes can be classified as ischemic (caused by a blood clot occluding vasculature in the brain thus impeding blood flow and tissue death), hemorrhagic (bleeding in the brain) or TIA (transient ischemic attack – a “mini-stroke” with symptoms resolving within 24 hours of symptom onset). TIAs are predictors of future strokes. • Stroke is the 3rd leading cause of death in MA and in the US. • Stroke is one of the leading causes of disability in the US. • While 83% of stroke patients are ambulating prior to their stroke hospitalization, only 51% are ambulating at the time of discharge. • For those suffering a hemorrhagic stroke, the change is from 75% prior to 28% post stroke. • Half of stroke patients are discharged home, a quarter are discharged to another hospital or long term care facility, 6% expire, and 20% are discharged to a rehab facility • 60% of stroke patients receive some degree of rehabilitation during their hospital stay.
Paul Coverdell Acute Stroke Registry DataCases discharged between December 2009 – November 2010 Source: MA Paul Coverdell Acute Stroke Registry, Data accessed February 2010 for the time period December 2009 – November 2010. Contact: katrina.damore@state.ma.us Heart Disease and Stroke Prevention and Control Program.
Brain Injury Symptom Surveillance Data • Maintained by MA Department of Public Health • One question on Youth Health Survey relative to youth reporting symptoms of head injury
Emergency Department Discharge Rates for Sports-related1 Traumatic Brain Injuries, MA Residents, FY2008 MA youth between the ages of 10 and 19 accounted for 77% of all sports-related TBIs treated in the ED (N=2,655). Source: MA Emergency Department Discharge Database, MA Division of Health Care Finance and Policy. 1 Includes only cases with E-codes (E886.0, E917.0, E917.5); other sports-related cases not receiving these codes are not included.
Percentage of Massachusetts Students1 Reporting Symptoms of a TBI2 While Playing with a Sports Team in the Past 12 months, (MA Youth Health Survey, 2009) 1 Includes only students who played on a sports team in the past 12 months. 2 Reported they suffered a blow or jolt to head while playing with a sports team (during a game or practice) which caused them to get "knocked out", have memory problems, double or blurry vision, headaches or "pressure" in the head or nausea or vomiting.
National TBI Estimates and Statistics • Each year, an estimated 1.7 million people sustain a TBI annually.1 • Of them: • 52,000 die, • 275,000 are hospitalized, and • 1.365 million, nearly 80%, are treated and released from an emergency department. • TBI is a contributing factor to a third (30.5%) of all injury-related deaths in the United States.1 • About 75% of TBIs that occur each year are concussions or other forms of mild TBI.2 • *The number of people with TBI who are not seen in an emergency department or who receive no care is unknown. Source: CDC, 2010, http://www.cdc.gov/traumaticbraininjury/statistics.html, 1. Faul M, Xu L, Wald MM, Coronado VG. Traumatic brain injury in the United States: emergency department visits, hospitalizations, and deaths. Atlanta (GA): Centers for Disease Control and Prevention, National Center for Injury Prevention and Control; 2010. 2. Centers for Disease Control and Prevention (CDC), National Center for Injury Prevention and Control. Report to Congress on mild traumatic brain injury in the United States: steps to prevent a serious public health problem. Atlanta (GA): Centers for Disease Control and Prevention; 2003.
National Statistics by Age and Gender TBI by Age1 • Children aged 0 to 4 years, older adolescents aged 15 to 19 years, and adults aged 65 years and older are most likely to sustain a TBI. • Almost half a million (473,947) emergency department visits for TBI are made annually by children aged 0 to 14 years. • Adults aged 75 years and older have the highest rates of TBI-related hospitalization and death. TBI by Gender1 • In every age group, TBI rates are higher for males than for females. • Males aged 0 to 4 years have the highest rates of TBI-related emergency department visits, hospitalizations, and deaths. Source: http://www.cdc.gov/traumaticbraininjury/statistics.html, 1. Faul M, Xu L, Wald MM, Coronado VG. Traumatic brain injury in the United States: emergency department visits, hospitalizations, and deaths. Atlanta (GA): Centers for Disease Control and Prevention, National Center for Injury Prevention and Control; 2010.
Conclusion • We have a patchwork picture of prevalence of TBI in MA • We have an incomplete picture of prevalence of ABI due to focus on TBI in data • Trends in hospital / ED usage are difficult to interpret due to increased awareness around brain injury, especially with sports related injuries
Where do we go from here? • What do we need to know about this population to move conversation forward? • What potential sources may be out there? • What recommendations would we make relative to improved data on brain injury population?