Download
1 / 1
10 likes | 157 Views
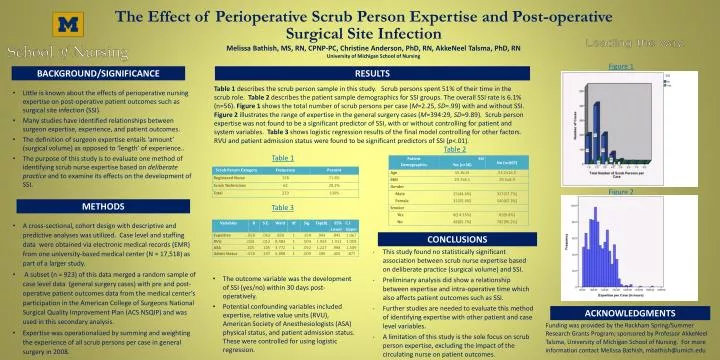
The Effect of Perioperative Scrub Person Expertise and Post-operative Surgical Site Infection. Melissa Bathish, MS, RN, CPNP-PC, Christine Anderson, PhD, RN, AkkeNeel Talsma, PhD, RN University of Michigan School of Nursing. Figure 1. BACKGROUND/SIGNIFICANCE. RESULTS.

E N D
The Effect of Perioperative Scrub Person Expertise and Post-operative Surgical Site Infection Melissa Bathish, MS, RN, CPNP-PC, Christine Anderson, PhD, RN, AkkeNeel Talsma, PhD, RN University of Michigan School of Nursing Figure 1 BACKGROUND/SIGNIFICANCE RESULTS • Table 1 describes the scrub person sample in this study. Scrub persons spent 51% of their time in the scrub role. Table 2 describes the patient sample demographics for SSI groups. The overall SSI rate is 6.1% (n=56). Figure 1 shows the total number of scrub persons per case (M=2.25, SD=.99) with and without SSI. Figure 2 illustrates the range of expertise in the general surgery cases (M=394:29, SD=9.89). Scrub person expertise was not found to be a significant predictor of SSI, with or without controlling for patient and system variables. Table 3 shows logistic regression results of the final model controlling for other factors. RVU and patient admission status were found to be significant predictors of SSI (p<.01). • Little is known about the effects of perioperative nursing expertise on post-operative patient outcomes such as surgical site infection (SSI). • Many studies have identified relationships between surgeon expertise, experience, and patient outcomes. • The definition of surgeon expertise entails ‘amount’ (surgical volume) as opposed to ‘length’ of experience.. • The purpose of this study is to evaluate one method of identifying scrub nurse expertise based on deliberate practice and to examine its effects on the development of SSI. Table 2 Table 1 Figure 2 METHODS Table 3 • A cross-sectional, cohort design with descriptive and predictive analyses was utilized. Case level and staffing data were obtained via electronic medical records (EMR) from one university-based medical center (N = 17,518) as part of a larger study. • A subset (n = 923) of this data merged a random sample of case level data (general surgery cases) with pre and post-operative patient outcomes data from the medical center’s participation in the American College of Surgeons National Surgical Quality Improvement Plan (ACS NSQIP) and was used in this secondary analysis. • Expertise was operationalized by summing and weighting the experience of all scrub persons per case in general surgery in 2008. CONCLUSIONS • This study found no statistically significant association between scrub nurse expertise based on deliberate practice (surgical volume) and SSI. • Preliminary analysis did show a relationship between expertise and intra-operative time which also affects patient outcomes such as SSI. • Further studies are needed to evaluate this method of identifying expertise with other patient and case level variables. • A limitation of this study is the sole focus on scrub person expertise, excluding the impact of the circulating nurse on patient outcomes. • The outcome variable was the development of SSI (yes/no) within 30 days post-operatively. • Potential confounding variables included expertise, relative value units (RVU), American Society of Anesthesiologists (ASA) physical status, and patient admission status. These were controlled for using logistic regression. ACKNOWLEDGMENTS Funding was provided by the Rackham Spring/Summer Research Grants Program; sponsored by Professor AkkeNeelTalsma, University of Michigan School of Nursing. For more information contact Melissa Bathish, mbathish@umich.edu