Download
1 / 15
190 likes | 920 Views
Osteoporosis. Debilitating disease in which bones become fragile and are more likely to break. It affects more than 28 million Americans, 80% of whom are women. Risk factors:

E N D
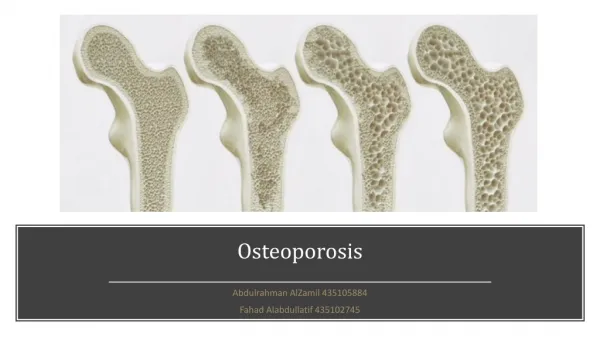
Osteoporosis • Debilitating disease in which bones become fragile and are more likely to break. It affects more than 28 million Americans, 80% of whom are women. • Risk factors: Gender- women are more likely to develop than men due to thinner, lighter bones & the decrease in estrogen production that occurs during menopause. Age- the longer you live, the greater the likelihood of developing.
Osteoporosis • Family history-is due part to heredity. • Ethnicity-Caucasian & Asian women are at highest risk;African-American & Hispanic women at lower but significant risk. • Body size- low body weight (< 127 lbs.) & a small-boned frame place at increased risk. • Lifestyle- a diet low in CA, inadequate vitamin D, little or no exercise, current cigarette smoking or excessive use of alcohol are all risk factors.
Osteoporosis • Assessment: Assess for backache with pain radiating around trunk Evaluate for skeletal deformities. Assess for pathologic fractures. Evaluate lab finding: 1. Serum CA, phosphorus & alkaline phosphatase are usually normal. 2. Parathyroid hormone may be elevated.
Osteoporosis • Diagnostic tests: 1. Routine x-ray when there is 25 to 45% demineralization. 2. Single-photon absorptionmetry identifies degree of bone in wrist. 3. Dual-photon absorptionmetry identifies bone loss at hip or spine
Osteoporosis • Nursing Diagnoses: 1. Risk for injury-altered mobility, minimal trauma, falls, advanced age, previous fall. 2. Impaired physical mobility- decreased bone mass, decreased strength, musculoskeletal impairment, pain. 3. Situational low self-esteem- chronic illness,anxiety, loss of usual role, body changes, limitation in mobility, chronic pain, loss of independence.
Osteoporosis • Prevention- by age 20, the average woman has acquired 98% of her skeletal mass. Building strong bones during childhood & adolescence can be the best defense against developing osteoporosis. 1. Balanced diet rich in CA & Vitamin D. 2. Weight-bearing exercises 3. A healthy lifestyle with no smoking & limited alcohol intake. 4. Bone density testing & medication when appropriate.
Osteoporosis • Prevent fractures: 1. Instruct in safety factors-watch steps, avoid use of scatter rugs. 2. Keep side rails up to prevent falls. 3. Move gently when turning & positioning. 4. Assist with ambulation if unsteady on feet. • Provide pain control. • Instruct in good use of body mechanics. • Provide diet high in protein, vit. D; avoid excessive use of alcohol & coffee.
Osteoporosis • Administer medications: 1.Estrogen & progesterone-decrease rate of bone reabsorption at menopause. 2. Calcium& vitamin D-support bone metabolism. • Instruct in regular exercise program. 1. ROM exercise 2. Ambulation several times per day.
Osteomalacia (adult rickets) • Metabolic bone disorder characterized by inadequate mineralization of bone matrix. Bone mineralization requires adequate calcium & phosphate ions in extracellular fluid. When either of these ions are insufficient because (1) inadequate CA intake or decreased CA absorption from intestines d/t insufficient Vit. D or (2) increased renal losses or decreased intestinal absorption of phosphate the bony matrix is not mineralized & thus unable to sustain weight bearing. Marked deformities of wt. Bearing bone & pathological fractures occur. Can be corrected with treatment.
Osteomalacia • Incidence: Health problem in cultures which tend to be deficient in calcium & vitamin D. Almost non existent in the U.S.-many foods are fortified with Vitamin D. Increased incidence in elders, very low birth weight infants, strict vegetarian. • Primary Causes in U.S.- Vitamin D deficiency- decreased intake, absorption, impaired renal tubular reabsorption d/t acquired or genetic disorders-most common cause alcohol abuse.
Osteomalacia • Assessment: 1. Bone pain- vague & generalized first, becoming more intense with activity as the disease progresses, occurs most frequently in the pelvis, long bones of extremities, spine & ribs. 2. Difficulty changing from lying to sitting position, sitting to standing. 3. Muscle weakness, waddling gait, dorsal kyphosis (severe), pathological fractures.
Osteomalacia • Assessment: 1. X-rays- effects of generalized bony demineralization-trabecular bone loss, cyst formation, compression fracture, bowing & bending deformities of the long bones, osteoid defosits (vertebral bodies/pelvis). Looser’s lines or zones-pseudofractures-they represent stress fx. that have not mineralized. They often appear symmetrically in the inner femora, ribs, & inferior pubic rami & may progress to complete fx. with minimal trauma.
Osteomalacia • Serum calcium-normal or low depending on cause • Serum phosphorus- typically is low may be up –renal failure. • Serum parathyroid hormone (PTH)-elevated as a compensatory response to hypocalcemia in client with renal failure or vitamin D deficiency.
Osteomalacia • Pharmacology- Vitamin D therapy-only if not enough with diet- 10ug or 400 IU to 600-800 IU. Fortified milk. • Nursing Diagnoses: 1. Alteration in nutrition < body requirements. 2. Risk for injury- evaluate home for hazards. PT consult-assistive devices. 3. Impaired physical mobility-conserve energy,gait devices, get brief exposure to sun.