Download
1 / 31
310 likes | 641 Views
Tuberculous and Fungal Infection of the Pleura. GENERAL THORACIC SURGERY CHAPTER 60. Tuberculous and fungal infection of the pleura. Pleural tuberculosis– Most often a side phenomenon of primary infection. Fungle empyema– Occurred in residule pleural space. .

E N D
Tuberculous and Fungal Infection of the Pleura GENERAL THORACIC SURGERY CHAPTER 60
Tuberculous and fungal infection of the pleura • Pleural tuberculosis– Most often a side phenomenon of primary infection. • Fungle empyema– Occurred in residule pleural space.
Tuberculous and fungal infection of the pleura • General guide line: First: Clean gross contamination (1). Tube thoracostomy. (2). Open window thoracostomy. Second: Obliteration the space.
Tuberculous and fungal infection of the pleura • The common feature of chronic mycobacterial and fungal infection–Underlying lung cannot be expanded to fill the pleural space because the partial resection or diffuse fibrosis.
Tuberculous and fungal infection of the pleura • Tuberculous empyema. • Aspergilus empyema. • Miscellaneous condition.
Pleural tuberculosis • Subdivided into three groups: 1. Primary TB, pleural effusion– 8%, serofibrinous, called tuberculous pleuritis. 2. Reaction TB, pleural infection turn to true empyema, opaque purulent effusion, pure or mixed. 3. Late complication of collapse therapy for TB.
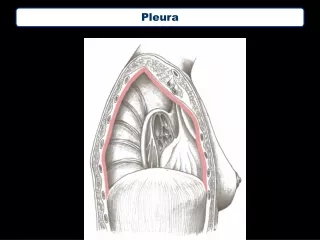
Tuberculous pleuritis • Pleural space– The second most common site of extrapulmonary TB(The first is lymphatic system.). • Originate– Subpleural pulmonary lesion.
Tuberculous pleuritis • Symptom/Sign: Lower grade fever, Weakness, Weight loss, Night sweat, Nonproductive cough, Pleuritic chest pain, Dyspnea.
Tuberculous pleuritis • Dignosis— • Chest x-ray—pleural effusion, 1/3 with concomitant parenchymal disease. • Tuberculin test– Early stage positive: 75%. • Pleural fluid– Exudates, protein excess 40 g/L, WBC 1-6 g/L with predominant lymphocyte, absence desquamated mesothelial cell. • Culture– 3-6 weeks. • IgG to mycobacterial antigen: 60, with cut-off value 150 u/ml. • Pleural biopsy: Most reliable. VATS. Histology– Caseating epithelioid granulomas is indicative of TB.
Tuberculous pleuritis • Treatment— • Antituberculous treatment, repeat thoracentesis, close observation. • Excessive production of exudative material– May start diffuse thickening the visceral pleura leading entrapment of the lung, regardless adequate antituberculous treatment. • Decortication should be considered.
Tuberculous pleuritis • PA view– are seen with pleural disease but not lateral view, the disease may progressive clear. • PA with lateral view were both seen pleural disease– The decortication should be considered.
Tuberculous pleuritis • Chest CT– Determination of appropriate timing of surgical intervention—Langston criteria—for DECORTICATION. 1. Thoracentesis fail to yield fluid or fail to alter radiographic apperance. 2. Pleural involvement 1/3 or 1/4 of hemithorax. 3. As early as is consistent with good judgement. (After 2-4 months of drug therapy). ● Generous Thoracotomy. ● VATS.
Tuberculous empyema • Patient didn’t receive major antituberculous drug therapy, chronic empyema by bronchopleural fistula, leading so-called mixed empyema.
Tuberculous empyema • Diagnosis—Lower grade fever, dyspnea, chest pain, abundant sputum. • Chest x ray—Increase extent of pleural involvement, air-fluid level. • Thoracentesis.
Tuberculous empyema • Treatment—Adequate drainage by tube thoracostomy, table 60-1. • First– Determine the underlying lung is re-expandable. • Second– Determine whether the parenchymal resection is required.
Tuberculous empyema • Indication of parenchymal resection: 1. Multiple drug resistant. 2. Threat hemoptysis. 3. Infection complication(Bronchiectasis or Aspergilloma). • Criteria for drug resistant: 1. Clinical or radiologic evidence of progressive disease. 2. Persistent mycobacteria on sputum examination after 3 months of a four-drug treatment. • The remaining lung is extensively destroy– Extrapleural pneumonectomy is considered.
Late pleural and extrapleural complications of Collapse therapy • Collapse therapy—Before early 1960. Only active treatment of TB. Collapse cavitated lung tissue, to obtain progressively scarring of the tuberculous area. • Fist stage– Creation artificial intrapleural pneumothorax: Injection air into pleural cavity q2 weeks, continue 2-3 years, the space progressively filled with serous fluid and retracted to a small and permanent residule space. • Second stage– Extramusculoperiosteal plombage called birdcage operation– The periosteum and intercostals muscle were stripped off the ribs, pushed inside the chest cavity. • Maintained with methyl mathacrylate ball.
Late pleural and extrapleural complications of collapse therapy • Side effect of collapse therapy—Many infectious complication, migrations of material. • All the procedure vanished with antibtuberculous chemotherapy. • Treatment– Decortication, re-expand the underlying lung, triple drainage connect to strong suction(100-150 mmhg), antituberculous therapy.
Aspergillous empyema • Aspergillous fumigatus. • Infrequent. • Fungal growth required persistent pleural space, temperature 370c, moisture 100%, abundant protein. • Acute and chronic.
Acute aspergillous empyema • Immediate postoperative course. • Most common is partial lung resection– Lobectomy or Segmentectomy.
Acute aspergillous empyema • Symptom /Sign— Prolonged air leak. Persistent drainage of fluid. Fever. Weight loss.
Acute aspergillous empyema • Diagosis– • Chest x ray: Residule space, rapid increase pleural air-fluid level, mediastinum shift. • CT. • WBC increase, CRP. • Analysis of pleural fluid. • Serodiagnosis.
Acute aspergillous empyema • Treatment— • Sterilization and complete obliteration of pleural space. • Antifungal therapy(itraconazole, amphotericin B, ). • Thoracoplasty.
Chronic aspergillous empyema • Residual pleural space with communicating with bronchial tree. • Most frequent in partial lung resection for TB or lung cancer. • Medical treatment with Itraconazole fail: Fibrotic scar tissue– Drug penetrating low, infection persistent as the residual space exist.
Chronic aspergillous empyema • Symptom /Sign— • Hemoptysis. • Bronchorrhea. • Dyspnea. • Chest pain.
Chronic aspergillous empyema • Diagosis— • Chest x-ray: Hydropneumothorax. • Direct identification of aspergillus species. • Serodiagnosis– Most reliable.
Chronic aspergillous empyema • Treatment— • Decortication– Easy fail. • Muscle transfer. • Curettage of all fungal material. • Thoracoplasty– Retailoring chest wall. • Mortality: 7%-- Infection, perioperative bleeding because of hypervascularization.
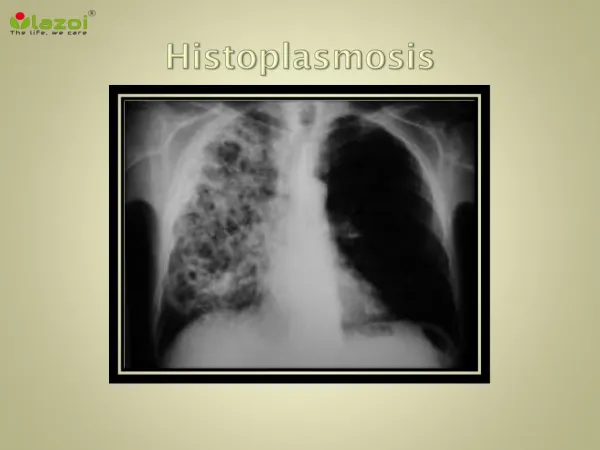
Miscellaneous conditions • Blastomycosis. • Histoplasmosis. • Cryptococcosis. • Sporotrichosis. • Treatment– Adequate antifungal therapy.
Coccidioidomycosis • Diffuse lung destruction. • 40%-- Acute infection as influenza-like. • 5%-- Irreversible pulmonary lesion as cavitation or bronchiectasis, • Treatment— Amphotericin B. • Surgical intervention– Bronchopleural fistula, chronic empyema, hemoptysis– Completion pmeumonectomy and mass closure of hilar vessel.
Candida empyema • Esophageal fistula. • Pneumonectomy: 0.5% with esophageal fistula. • Intraoperative injury, devascularization with subsequent necrosis. • Diagnosis—Contrast study. • Treatment—Chest tube, direct repair the esophagus with reinforced with myoplasty and omentoplasty, thoracoplasty or muscle flap transfer.