Download
1 / 15
160 likes | 304 Views
Transmission. • Sexual transmission via the vagina & cervix • Gynecological surgical procedures • Child birth/ Abortion • A foreign body inside uterus (IUCD). Transmission. • Contamination from other inflamed structures in abdominal cavity

E N D
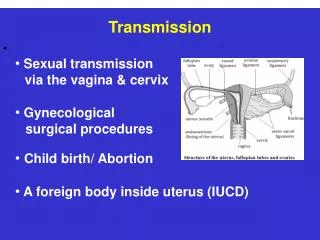
Transmission • • Sexual transmission • via the vagina & cervix • • Gynecological • surgical procedures • • Child birth/ Abortion • • A foreign body inside uterus (IUCD)
Transmission • • Contamination from • other inflamed structures • in abdominal cavity • (appendix, gallbladder) • • Blood-borne transmission • (pelvic TB)
Definitive Criteria (CDC 2002) • Endometrial biopsy with histopathology evidence of endometritis • TVS/ MRI: Thickened fluid filled tubes/ free pelvic fluid / tubo-ovarian complex • Laparoscopic abnormalities consistent with PID
When should treatment be stopped ? • Parenteral changed to oral therapy after 72 hrs, if substantial clinical improvement • Continue Oral therapy until clinical & biological signs (leukocytosis, ESR, CRP) disappear or for at least 14 days • If no improvement, additional diagnostic tests/ surgical intervention for pelvic mass/ abscess rupture
Associated treatment Rest at the hospital or at home Sexual abstinence until cure is achieved Anti-inflammatory treatment Dexamethasone 3 tablets of 0.5 mg a day or Non steroidal anti-inflammatory drugs Oestro-progestatives: contraceptive effect + protection of the ovaries against a peritoneal inflammatory reaction + cervical mucus induced by OP has preventive effect against re-infection.
Special Situations Pregnancy - Augmentin or Erythromycin - Hospitalization Concomitant HIV infection - Hospitalization and i.v. antimicrobials - More likely to have pelvic abscesses - Respond more slowly to antimicrobials - Require changes of antibiotics more often - Concomitant Candida and HPV infections
Surgery in PID Indications Acute PID -Ruptured abscess - Failed response to medical treatment - Uncertain diagnosis Chronic PID - Severe, progressive pelvic pain - Repeated exacerbations of PID - Bilateral abscesses / > 8 cm. diameter - Bilateral uretral obstruction
Management of sex partners • Examination and treatment if they had sexual contact with patients during the 60 days preceding the onset of symptoms in the patients. • Empirical treatment with regimens effective against C. trachomatis and N. gonorrhoeae
Prevention • Primary Prevention: • - Sexual counseling: practice safe sex, limit the number of partners, avoid contact with high-risk partners, delay the onset of sexual activity until ≥ 16 years. • - Barrier and Oral contraceptives reduce the risk for developing PID. • Secondary Prevention: • • - Screening for infections in high- risk. • - Rapid diagnosis and effective treatment of STD and lower urinary tract infections. • Tertiary Prevention: • -Early intervention & complete treatment.