Download
1 / 43
430 likes | 578 Views
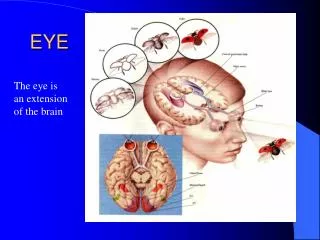
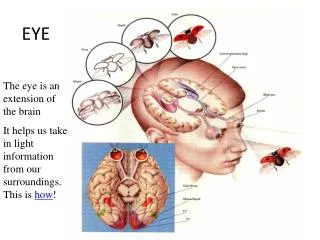
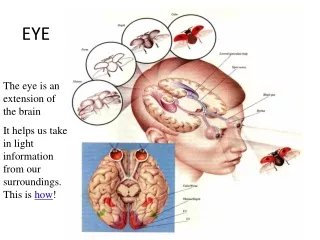
EYE. ** External Anatomy:. eye is the sensory organ of vision. Protected by the bony orbital cavity, with a cushion of fat, eyelids & lashes protect the eye from injury, light& dust. palpebral fissure (distance between lid margins).page 298:. EYE. External Eye Structures.

E N D
** External Anatomy: • eye is the sensory organ of vision. Protected by the bony orbital cavity, with a cushion of fat, eyelids& lashes protect the eye from injury, light& dust. palpebral fissure (distance between lid margins).page 298:
EYE • External Eye Structures Figure 12-1. p. 298.
Lacrimal Apparatus • Irrigates & moisturizes the conjunctiva and the cornea • Gland – secretes tears • Puncta- where tears drain • Nasolacrimal duct- empties into the nose
Conjunctiva • Transparent protective covering • Thin mucous membrane folded like an envelope • Palpebral- clear, lines the lids • Bulbar – overlays the eyeball
Lacrimal Apparatus • Irrigates & moisturizes the conjunctiva and the cornea • Gland – secretes tears • Puncta- where tears drain • Nasolacrimal duct- empties into the nose
Lacrimal Apparatus Figure 12-3. p. 299.
Extraocular muscles: • six muscles attach the eye ball to its orbit. 4 straight or rectus muscles are superior, inferior, lateral & medial, 2 oblique are superior & inferior muscles. Each one coordinated with one in the other eye. So when two eyes move their axes always remain parallel.
Extraocular muscles:cont • Movement of Extraocular muscles stimulated by 3 cranial nerves • CN VI abducens innervate lateral rectus muscle • CN IV trochlear innervate superior oblique muscle • CN III oculomotor innervate the sup, inf & medial rectus &inferior oblique muscles.
** Internal Anatomy: • Outer layer:sclera it’s a protective white covering, cornea bending light rays to focused on inner retina- cornea sensitive to touch(corneal reflex)-trigeminal nerve(CN V) carries afferent sensation into brain, facial nerve(CN VII) carries efferent messages that stimulates the blink.
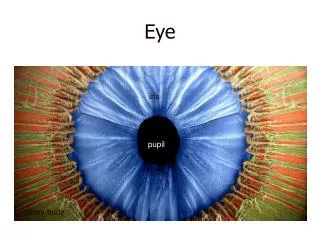
Middle layer: • choroids has dark pigmentation to prevent light from reflecting internally- continues with iris ( varying opening at its center, the pupil ).so controls the amount of light admitted into retina. • Pupil: round & regular size according to nervous system. • lens is a biconvex disc located posterior to pupil serves as a refracting medium keeping object on retina(bulges on near objects& flattens for far objects)- • anterior chamber posterior to cornea contain aqueous humor to deliver nutrients to surrounding tissues & drains metabolic waste.
Inner layer: • retina ; the visual receptive layer which light waves are changed into nerve impulses- • optic disc is the area in which fibers from the retina converge to form the optic nerve color varies from yellow-orange to pink around or oval shape , physiologic cup →blood vessels exit&enter– • macula located on temporal side of the fundus, darker pigmented surrounding • fovea centralis(area of sharpest vision) receives & transduce light from visual field center.
Aging Adult • Lacrimal glands involute –↓tear production • Pupil size ↓ • Lens becomes hard & glasslike causing presbyopia (farsighted) • Cataract formation – (lens opacity) • Glaucoma –↑ocular pressure • Macular degeneration – Loss of central vision, most common cause of blindness
** Visual Pathways & visual Fields: • objects reflect right, refracted through the transparent media(cornea → aqueous humor→ lens → vitreous body)& strike retina. Retina transforms light stimulus into nerve impulses that are conducted through optic nerve & optic tract to visual cortex of occipital lobe.
The image formed on the retina is upside down & reversed. Left optic tract has fibers from lt half of each retina& rt optic tract contains fibers only from rt. thus rt side of brain looks at lt side of the world.
** Visual Reflexes: # papillary light reflex: is a normal constriction of pupil when light shines on retina( a direct reflex & a consensual reflex). Page 302(14-8) • Mechanism: light →retina → optic Nerve(II)__ efferent or sensory → midbrain(Rt <) → CN III (oculomotor) _ afferent(motor) → constriction of iris muscles for both eyes. • Direct reflex → same eye _Consensual reflex → opposite eye.
# Accommodation: adaptation of the eye for near vision, by increasing curvature of lens. Pupil constricted+ motion toward axes of eyeball.
** Subjective Data: 1)vision difficulty(decreased acuity, blurring, blind spots) – come on sudden or progressed slowly , in one eye or both?- any halos around objects? or rings around light? any night blindness? 2) Pain: Quality- itching? sharp, stabbing? 3) Strabismus, diplopia: hx of crossed eyes? Ever see double? constant or come and go? In one eye or both? 4) Redness, swelling: any infections? when? are they seasonal? 5) Watering, discharge: excessive tearing- discharge what color?
** Subjective Data: cont 6)Past hx of ocular problems: injury or surgery to eye? Allergies? 7) Glaucoma: ever been tested for it? Family hx? 8) Use of glasses or contact lenses: last time you checked? any problems? as pain, photophobia ?how you care for contacts? 9) Self-care behaviors: last vision test, do you wear glasses to protect eyes? 10) Medications?
** Objective Data: • preparation: position person sitting up with head at your eye level. • Equipment needed: snellen chart- card penlight- ophthalmoscope.
** INSPECT EXTERNAL OCULAR STRUCTURES: • start most external to inward . # general: persons ability to move around room, avoid obstacles, respond to your directions # Eyebrows: bilaterally present, move symmetrically, no scaling or lesions. # eyelids & lashes: upper lids normally overlap sup part of iris &lower lids when closed, no redness, swelling, discharge, or lesions. evenly distributed & curve outward. # eyeballs: no protrusion or sunken appearance
# Conjunctiva & sclera: • ask person to look up. using your thumbs , slide the lower lids down ,inspect exposed area moist , clear, pink over lower lids & white over sclera, note color change, swelling, or lesions. sclera is shining white, blacks have gray-blue color & small brown macules, also yellowish fatty deposits beneath lids away from cornea.
# lacrimal apparatus: • ask person looks down, with your thumbs, slide outer part of upper lid up along the bony orbit, inspect for any redness or swelling, presence of excessive tearing may indicate blockage of nasolacrimal ducts, check by pressing index against sac inside lower orbital rim, not against side of nose.
** INSPECT ANTERIOR EYEBALL STRUCTURES: • # cornea & lens: shine a light from a side across cornea& check for smoothness& clarity, should be no cloudiness. • -with aging → a gray-white arc around limbus due to fat deposition
# Iris & pupil: iris flat, round regular & even color, pupil round, regular& indicator both pupil 3 mm & constrict to light to 1 mm. for accommodation: ask person to focus on a distant object ,this dilates pupil then make him shift gaze to a near object, a normal response : pupilary constriction+ convergence of axes of eyes, record as PERRLA, or Pupil Equal Round React To Light & Accommodation.
* VISUAL ACUITY: # Snellen Chart: accurate measure of visual acuity, have lines of letters arranged in decreasing size( or E chart). Place chart at eye level 20 feet in between, hand person card to shield one eye at a time, if he wear glasses or lenses leave them on. Record the result using numeric fraction at the end of last successful line read. Normal 20/20, top no indicates the distance person standing from chart, while denominator gives distance at which a normal eye could have read that particular line.
Snellen Chart: cont if he is unable to see even the largest letter, shorten the distance until its seen & record distance(10/100), if lower → let him count your fingers after spreading them.
# Near Vision: • people over 40 year test near vision using a handheld screen with various sizes of print. let him read from magazine.
** TEST VISUAL FIELDS: # confrontation test: a gross measure of peripheral vision. Its compares his with your own. Position at eye level2 feet away, cover one eye with a card, other eye look straight at you, cover your own eye opposite to his. hold a pencil or finger as a target midline between you & him, slowly advanced it from the periphery in several directions. Ask person to say “now” as he first seen. which should be as you see it also. Normal results are 50 degrees upward, 90 degree temporal, 70 degree down, 60 degree nasal.
** INSPECT EXTRAOCULAR MUSCLE FUNCTION: # Corneal light reflex(Hirschberg test): • assess parallel alignment of eye axes by shining a light towards person eyes. Direct him to stare straight ahead as you hold light 30 cm away. note reflection of the light on corneas it should be in exactly same spot on each eye
# Cover test: • detects small degrees of deviated alignment by interrupting fusion reflex that normally keeps the two eyes parallel. ask him to stare straight ahead at your nose, cover one eye note uncovered one a normal response is a steady fixed gaze. if muscle weakness exist the covered eye will drift into a relaxed position, then uncover the eye & observe it for movement, it should stare straight ahead. if it reestablish fixation eye muscle weakness exists, repeat with other eye.
# Diagnostic positions test: • ask person to hold head steady & to follow the movement of your finger only with eyes. Back 12 inch move it to 6 positions, progress clockwise, a normal response is parallel tracking of object with both eyes, note any nystagmus, note upperlid continues to overlap superior part of iris even during downward movement, you should not see a white rim of sclera between the lid & iris if noted termed “lid lag”.
** INSPECT THE OCULAR FUNDUS: • ophthalmoscope contains a set of lenses control focus, the unit of strength of each lens is the diopter, black numbers indicate a positive diopter, focus on objects near in space , red numbers show a negative diopter & focusing on objects farther away. darken the room to dilate pupil, if pupil small use smaller white light, light must have maximum brightness, tell him “please keep looking at the light switch”, even though my head will get in the way.
Hold ophthalmoscope in your right hand up to your rt eye to view person’s rt eye, place your free hand on person’s shoulder or forehead. • Begin about 25 cm away from the person at an angle 15 degree lateral to person’s line of vision. Note red glow filling the person’s pupil, this is red reflex, keep sight of red reflex &steady move closer to eye, as you advance, adjust lens to +6 & note any opacities in the media.
Progress toward person until your forehead almost touch. at normal vision diopter at zero, use red lenses for nearsighted eyes& black for farsighted eyes. Moving in on 15 degree lateral line , symmetrically inspect structures as optic disc- retinal vessels- background- macula.
# optic disc: • nasal side of retina, explore these characteristics: 1- color : creamy yellow –orange to pink 2- shape: round or oval 3- margins: distinct & demarcated 4- cup- disc ratio: varies, when visible, physiologic cup is a brighter yellow- white than rest of the disc, its width is not more than one half the disc diameter. - diameter disc DD is a standard measure.
# retinal vessels: • only place in body can view blood vessels , note these: 1- number: a paired artery & vein pass to each quadrant 2- color: arteries are brighter red than veins 3- A:V ratio: comparing artery to vein width is 2:3 or 4:5
# General background: color varies from light red to dark brown-red, clear, no lesions # Macula: • 1 DD in size, located in 2 DD temporal to the disc • inspect it last in exam • light on area causes watery & discomfort & pupilary constriction • color darker but even & homogenous • note foveal light reflex → a tiny white dot.