Download
1 / 1
10 likes | 178 Views
Is data quality more important than data quantity in the diagnosis of occupational asthma from serial PEF records? MOORE VC, BURGE CBSG, AND BURGE PS Occupational Lung Disease Unit, Birmingham Heartlands Hospital, UK. ABSTRACT. SERIAL PEF RECORD CHANGES AT EACH RANDOMISATION.

E N D
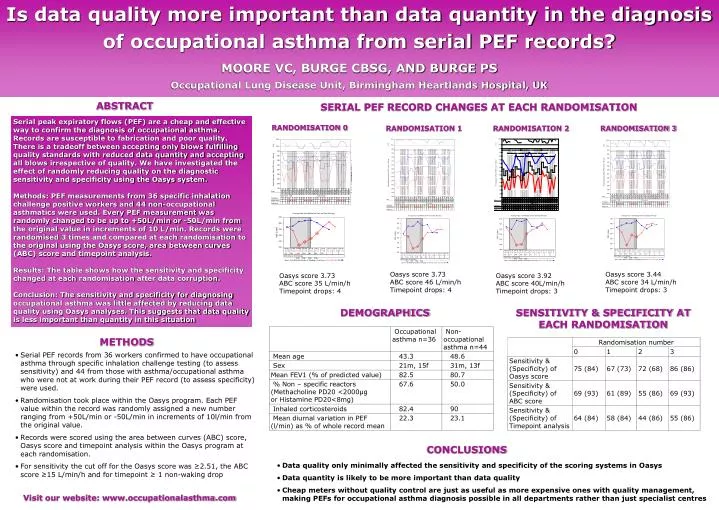
Is data quality more important than data quantity in the diagnosis of occupational asthma from serial PEF records? MOORE VC, BURGE CBSG, AND BURGE PS Occupational Lung Disease Unit, Birmingham Heartlands Hospital, UK ABSTRACT SERIAL PEF RECORD CHANGES AT EACH RANDOMISATION Serial peak expiratory flows (PEF) are a cheap and effective way to confirm the diagnosis of occupational asthma. Records are susceptible to fabrication and poor quality. There is a tradeoff between accepting only blows fulfilling quality standards with reduced data quantity and accepting all blows irrespective of quality. We have investigated the effect of randomly reducing quality on the diagnostic sensitivity and specificity using the Oasys system.Methods: PEF measurements from 36 specific inhalation challenge positive workers and 44 non-occupational asthmatics were used. Every PEF measurement was randomly changed to be up to +50L/min or -50L/min from the original value in increments of 10 L/min. Records were randomised 3 times and compared at each randomisation to the original using the Oasys score, area between curves (ABC) score and timepoint analysis.Results: The table shows how the sensitivity and specificity changed at each randomisation after data corruption. Conclusion: The sensitivity and specificity for diagnosing occupational asthma was little affected by reducing data quality using Oasys analyses. This suggests that data quality is less important than quantity in this situation RANDOMISATION 0 RANDOMISATION 1 RANDOMISATION 2 RANDOMISATION 3 Oasys score 3.73 ABC score 46 L/min/h Timepoint drops: 4 Oasys score 3.44 ABC score 34 L/min/h Timepoint drops: 3 Oasys score 3.73 ABC score 35 L/min/h Timepoint drops: 4 Oasys score 3.92 ABC score 40L/min/h Timepoint drops: 3 DEMOGRAPHICS SENSITIVITY & SPECIFICITY AT EACH RANDOMISATION METHODS • Serial PEF records from 36 workers confirmed to have occupational asthma through specific inhalation challenge testing (to assess sensitivity) and 44 from those with asthma/occupational asthma who were not at work during their PEF record (to assess specificity) were used. • Randomisation took place within the Oasys program. Each PEF value within the record was randomly assigned a new number ranging from +50L/min or -50L/min in increments of 10l/min from the original value. • Records were scored using the area between curves (ABC) score, Oasys score and timepoint analysis within the Oasys program at each randomisation. • For sensitivity the cut off for the Oasys score was ≥2.51, the ABC score ≥15 L/min/h and for timepoint ≥ 1 non-waking drop CONCLUSIONS • Data quality only minimally affected the sensitivity and specificity of the scoring systems in Oasys • Data quantity is likely to be more important than data quality • Cheap meters without quality control are just as useful as more expensive ones with quality management, making PEFs for occupational asthma diagnosis possible in all departments rather than just specialist centres Visit our website: www.occupationalasthma.com



















