Download
1 / 1
10 likes | 151 Views
1. Health 1.1 Health Outcomes 1.2 Quality Health service. 2. Organizational 2.1 Institutional Capacity 2.2 Organizational Viability. 3. Community & Ecological 3.1 Community Capacity 3.2 Ecological Situation. The Sustainability Assessment (CSSA) Framework.

E N D
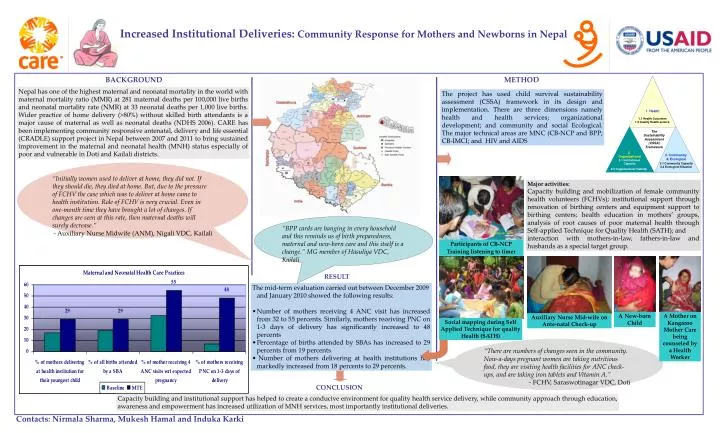
1. Health 1.1 Health Outcomes 1.2 Quality Health service 2. Organizational 2.1 Institutional Capacity 2.2 Organizational Viability 3. Community & Ecological 3.1 Community Capacity 3.2 Ecological Situation The Sustainability Assessment (CSSA) Framework Increased Institutional Deliveries: Community Response for Mothers and Newborns in Nepal BACKGROUND METHOD Nepal has one of the highest maternal and neonatal mortality in the world with maternal mortality ratio (MMR) at 281 maternal deaths per 100,000 live births and neonatal mortality rate (NMR) at 33 neonatal deaths per 1,000 live births. Wider practice of home delivery (>80%) without skilled birth attendants is a major cause of maternal as well as neonatal deaths (NDHS 2006). CARE has been implementing community responsive antenatal, delivery and life essential (CRADLE) support project in Nepal between 2007 and 2011 to bring sustained improvement in the maternal and neonatal health (MNH) status especially of poor and vulnerable in Doti and Kailali districts. The project has used child survival sustainability assessment (CSSA) framework in its design and implementation. There are three dimensions namely health and health services; organizational development; and community and social Ecological. The major technical areas are MNC (CB-NCP and BPP; CB-IMCI; and HIV and AIDS “Initially women used to deliver at home, they did not. If they should die, they died at home. But, due to the pressure of FCHV the case which was to deliver at home came to health institution. Role of FCHV is very crucial. Even in one-month time they have brought a lot of changes. If changes are seen at this rate, then maternal deaths will surely decrease.” - Auxiliary Nurse Midwife (ANM), Nigali VDC, Kailali Major activities: Capacity building and mobilization of female community health volunteers (FCHVs); institutional support through renovation of birthing centers and equipment support to birthing centers; health education in mothers’ groups, analysis of root causes of poor maternal health through Self-applied Technique for Quality Health (SATH); and interaction with mothers-in-law, fathers-in-law and husbands as a special target group. “BPP cards are hanging in every household and this reminds us of birth preparedness, maternal and new-born care and this itself is a change.” MG member of Hasuliya VDC, Kailali Participants of CB-NCP Training listening to timer RESULT • The mid-term evaluation carried out between December 2009 and January 2010 showed the following results: • Number of mothers receiving 4 ANC visit has increased from 32 to 55 percents. Similarly, mothers receiving PNC on 1-3 days of delivery has significantly increased to 48 percents • Percentage of births attended by SBAs has increased to 29 percents from 19 percents. • Number of mothers delivering at health institutions has markedly increased from 18 percents to 29 percents. A New-born Child A Mother on Kangaroo Mother Care being counseled by a Health Worker Auxiliary Nurse Mid-wife on Ante-natal Check-up Social mapping during Self Applied Technique for quality Health (SATH) “There are numbers of changes seen in the community. Now-a-days pregnant women are taking nutritious food, they are visiting health facilities for ANC check-ups, and are taking iron tablets and Vitamin A.” - FCHV, Saraswotinagar VDC, Doti CONCLUSION Capacity building and institutional support has helped to create a conducive environment for quality health service delivery, while community approach through education, awareness and empowerment has increased utilization of MNH services, most importantly institutional deliveries. Contacts: Nirmala Sharma, Mukesh Hamal and Induka Karki