Download
1 / 28
280 likes | 341 Views
Explore the mechanisms of action of steroids in treating Minimal Change Disease, its effectiveness, and potential direct effects on the kidneys. Discover key research findings on steroid therapy and its impact on podocyte function.

E N D
Minimal change disease and treatment with steroids 7/24/2007 Zae Kim, MD
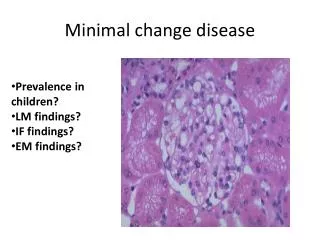
Clinical Question • Why does MCD respond to steroid? • Why do they develop resistance?
Introduction • Most common cause of the nephrotic syndrome in children • ~10-15% of nephrotic syndrome in adults, third most common after MN and FSGS • More common in Hispanics, Asians, Arabs and Caucasians • clinical and pathologicalentity defined by selective proteinuria and hypoalbuminemiathat occurs in the absence of • cellular glomerular infiltratesor • immunoglobulin deposits
Immunofluorescence Microscopy www.gamewood.net/rnet/renalpath/noimcx.jpg
The glomerular capillary wall Normal MCD Van den Berg, Weening, Clinical Science (2004) 107, 125–136
Pathogenesis - “Intrinsic factor” • Genetic basis for hereditary NS • NS of the Finnish type • Autosomal-recessive steroid-resistant NS • Familial forms of FSGS • Diffuse mesangila sclerosis associated with Denys-Drash syndrome and with Frasier syndrome • NS associated with nail-patella syndrome • Help elucidate molecular aspect of FSGS • Not clear for MCD
Molecular anatomy of the podocyte foot process cytoskeleton Nature Genetics24, 333 - 335 (2000)
Pathogenesis – extrinsic factor, better explanation for MCD • Clinical Observations - Shalhoub’s hypothesis • MCD frequently remits with measles infection • Corticosteroids and alkylating drugs cause a remission • Association of MCD with Hodgkin disease • Experimental Observations • T cell hybridoma (Koyama KI 1991 (40): 453-460) • Removal of glomerular permeability factor leads to normal kidney (Ali Transplantation 1994 Oct 15;58(7):849-52) • “circulating factor” • possible link between T-cell response and glomerular disease
How does steroid work in MCD? • Widely used in treatment but their mode of action is poorly understood • What is its effectiveness in MCD where there is no evident inflammation
Steroid – quick overview • Inhibitory effects on both innate and acquired immunologic function • Innate Immune function • Reduced Inflammatory response: • inhibit transmigration of leukocytes • attenuate the generation of inflammatory exudates • Phospholipase A2 suppresion • COX-2 suppression • Acquired Immune function • Antigen presenting cells, B cell and T cells
Direct effects of dexamethasone on human podocyte – Xing, Saleem, et al • Hypothesis: • Glucocorticoid exert direct protection of podocytes from injury and/or promotion of repair • Nephrin: podocyte specific protein • mutation of NPHS2 gene - cause congenital nephrotic syndrome of Finnish type • Studies show possible downregulation of nephrin in MCD
Result – effects of dexamethasone on podocyte maturation at 37 C and expression of nephrin Immunofluorescent staining Quantificaton of nephrin
Summary • Dexamethasone enhanced and accelerated podocyte maturation, with a particulary striking effect on expression of nephrin
Overexpression of Interleukin-13 Induces Minimal-Change–Like Nephropathy in Rats • Background • MCD may be a T cell dependent disorder that results in glomerular podocyte dysfunction • Th2 cytokine bias in patients with MCD • MCD associated with atopy and allergy • Relapse MCD with elevated IL-4 and IL-13 • Association between MCD and Hodgkins’s disease • IL-13 known to be an autocrine growth factorfor the Reed-Sternberg
Hypothesis • IL-13 may play an important role in the development ofproteinuria in MCNS by exerting a direct effect on podocytes,acting through the IL-13 receptors on the podocyte cell surface,initiating certain signaling pathways that eventually lead tochanges in the expression of podocyte-related proteins (nephrin, podocin, and dystroglycan) • IL-13 transfected mouse was used as a model
Comparison of control, IL-13-transfected mouse at experiment end (day 70) Yellow = p <0.001 vs control Red = p<0.001 vs control and Grp 1
Histopathologic features on day 70 at killing(A) Glomerulus of IL-13–transfected rat showing no significant histologic changes (periodic acid-Schiff stain). (B) Glomerulus of IL-13–transfected rat showing fusion of podocyte foot processes (arrows). (C) Glomerulus of control rat showing normal individual podocyte foot processes along the glomerular basement membrane (GBM; arrows).
Control IL-13 infected Immunofluorescence staining of glomeruli for protein expression of nephrin, podocin, dystroglycan, and synaptopodin nephrin podocin dystroglycan synaptopodin
Summary • IL-13-transfected rats • Developed minimal change like GN, as evidence by LM and EM changes • decrease in the expression of nephrin, podocin,and dystroglycan associated with increased urinary albumin excretion and podocytefoot process effacement • suggesting that these proteins areessential in maintaining the filtration barrier, thus controllingglomerular permeability • decrease was not due to loss ofpodocytes -
What does it all mean… • There is more to steroid than I knew… • “circulating factor” • Prognostic indicator? • Why are some MCDs steroid responsive while others are resistant?