Download
1 / 37
380 likes | 673 Views
Buynak Synopsis Vaccines. Medicinal Chemistry Donlene Mallon SMU. Viruses. A virus is a submicroscopic obligate parasitic particle that infects cells in biological organisms. Viruses are non-living particles that can only replicate when an organism reproduces the virulent RNA or DNA.

E N D
Buynak Synopsis Vaccines Medicinal Chemistry Donlene Mallon SMU
Viruses • A virus is a submicroscopic obligate parasitic particle that infects cells in biological organisms. • Viruses are non-living particles that can only replicate when an organism reproduces the virulent RNA or DNA. • Among other things, viruses do not move, metabolize, or decay on their own. Viruses are obligate intracellular parasites that lack the cellular machinery for self-reproduction. • Viruses infect eukaryotes and prokaryotes such as bacteria; bacteriophages. • Typically viruses carry a small amount of genetic material, either in the form of RNA or DNA, but not both, surrounded by some form of protective coat consisting of proteins, lipids, glycoproteins or a combination. • The viral genome codes for the proteins that constitute this protective coat, as well as for those proteins required for viral reproduction that are not provided by the host cell.
Viruses • Viral nucleic acid can be DNA or RNA. It can be single or double stranded, circular or linear, with most being linear. • The nucleic acid is protected from physical, chemical and enzymatic damage by a protein coat called a Capsid. • Many viruses have a second envelope surrounding the Capsid on which there are spikes with antigenic determinants. • This outer surface of the virus is responsible for host cell recognition. Initially viral proteins on the outer surface will attach to the hosts receptor molecules. A simplified viron is illustrated below.
Life Cycle ▪Attachment, sometimes called absorption: The virus attaches to receptors on the host cell wall. • Injection: The nucleic acid of the virus moves through the plasma membrane and into the cytoplasm of the host cell. The capsid of a phage, a bacterial virus, remains on the outside. In contrast, many viruses that infect animal cells enter the host cell intact. • Transcription: Within minutes of phage entry into a host cell, a portion is transcribed into mRNA, which is then translated into proteins specific for the infecting phage. • Replication: The viral genome contains all the information necessary to produce new viruses. Once inside the host cell, the virus induces the host cell to synthesize the necessary components for its replication. • Assembly: The newly synthesized viral components are assembled into new viruses. • Release: Assembled viruses are released from the cell and can now infect other cells, and the process begins again.
Vaccines • Take advantage of the immune system to kill disease-causing microbe • Have nearly eliminated diseases that killed hundreds of thousands of people in the 19th and early 20th century • Vaccines protect the whole community, since if your immune system is trained to kill a disease, you will not be contagious for long, thus you will not be able to spread the disease to unvaccinated individuals. • The word “vaccine” comes from the Latin word “vaccinus”, which means “pertaining to cows”
Origin of Vaccines Smallpox was the first disease people tried to prevent by purposely inoculating themselves with other types of infections. Inoculation is believed to have started in India or China before 200 BC. Physicians in China immunized patients by picking off pieces from drying pustules of a person suffering from a mild case of smallpox, grinding the scales to a powdery substance, and then inserting the powder into the person's nose in order for them to be immunized. In 1718, Lady Mary Wortley Montague reported that the Turks have a habit of deliberately inoculating themselves with fluid taken from mild cases of smallpox. Lady Montague inoculated her own children in this manner. In 1796, during the heyday of the smallpox virus in Europe, an English country doctor, Edward Jenner, observed that milkmaids would sometimes become infected with cowpox through their interactions with dairy cows' udders. Cowpox is a mild relative of the deadly smallpox virus. Building on the foundational practice of inoculation, Jenner took infectious fluid from the hand of milkmaid Sarah Nelmes. He inserted this fluid, by scratching or injection, into the arm of a healthy local eight year old boy, James Phipps. Phipps then showed symptoms of cowpox infection. Forty-eight days later, after Phipps had fully recovered from cowpox, Jenner injected some smallpox-infected matter into Phipps, but Phipps did not later show signs of smallpox infection
The Immune System • Usually takes more than a week to learn how to fight off an unfamiliar microbe • Certain microbes are so powerful (virulent) that they can overwhelm your body’s natural defenses • Once your immune system is trained to resist a disease, you are said to be ‘immune’ to it • When you get sick and (hopefully) recover, you receive “naturally acquired immunity” • Vaccines provide “artificially acquired immunity” and thus represent a less risky way to become immune
The Immune System: Macrophages • Macrophages: Literally “big eaters”, white blood cells that engulf foreign organisms. • Macrophages recognize what is foreign by identifying its “antigens” • Macrophages save the antigens, and carry them back to the lymph nodes, where immune system cells congregate • Macrophages show the antigens to specialized white blood cells, called lymphocytes
The Immune System: Lymphocytes • Lymphocytes swing into action when they see the foreign antigens • Lymphocytes Come in Two types: T Cells and B Cells • T Cells come in two types: cytotoxic T cells and helper T cells • Cytotoxic T cells are also called “killer” T cells. They latch onto the foreign invader and release chemicals that destroy it. • Helper T cells assist in activating killer T cells and also work with B cells • B Cells secrete antibodies secrete antibodies that bind to the antigens on the surface of the invader • Antibodies provide a signal to macrophages and other defensive cells to come and eat the invader.
The Immune System: Memory Cells • Following the disease, some of the defensive B cells and T cells are converted into memory cells. • Memory B cells can quickly divide into plasma cells and make more antibody if needed • Memory T cells can quickly divide and grow up into a disease fighting army.
Vaccines • Vaccines contain a weakened form of the microbe that doesn’t cause disease or reproduce • Vaccines stimulate the macrophages, which present the antigens to T and B cells • The mock infection is rapidly cleared, and you are left with a supply of memory T cells and B cells to protect you against of future infection of this type
One type of vaccine: Live attenuated vaccines • Live attenuated vaccines contain a version of the living organism that has been weakened the lab so it can’t cause disease • Since these vaccines are close to the actual infection, they elicit strong immune system responses and usually confer lifelong immunity with only one or two doses • Downside: live attenuated vaccines could potentially revert to a virulent form and cause disease. For this reason, they are not given to people with weakened immune systems (e.g. cancer patients, or those infected with HIV) • Downside: must be refrigerated to stay potent • Hard to create live attenuated vaccines to treat bacterial infections (since bacteria have thousands of genes and are harder to tame)
Live Vaccines 1. Live attenuated organisms • Organisms whose virulence has been artificially reduced by in vitro culture under adverse conditions, such as reduced temperature. This results in the selection of mutants which replicate poorly in the human host and are therefore of reduced virulence. Replication of the vaccine strain in the host reproduces many of the features of wild type infection, without causing clinical disease. Most successful viral vaccines belong to this group. • The immune response is usually good - when the virus replicates in the host cells, both antibody as well as cell mediated immune responses are generated and immunity is generally long lived. Often, only a single dose is needed to induce long term immunity.
Live Vaccines 3. Live recombinant vaccines • It is possible, using genetic engineering, to introduce a gene coding for an immunogenic protein from one organism into the genome of another (such as vaccinia virus). The organism expressing a foreign gene is called a recombinant. Following injection into the subject, the recombinant organism will replicate and express sufficient amounts of the foreign protein to induce a specific immune response to the protein. Attributes • Good immune response • Both Cell Mediated Immunity and antibody responses. • Immunity is long lived • Single dose • Safety • Danger of reversion to virulence, or • Severe disease in immunocomprised • Stability • Organisms in the vaccine must remain viable in order to infect and replicate in the host • Vaccine preparations are therefore very sensitive to adverse storage conditions • Maintenance of the cold chain is very important. • Expense • Cheap to prepare
Type of vaccine: Inactivated or killed vaccines • In inactivated vaccines, the disease-causing microbe is killed with chemicals, heat, or radiation • The dead microbes can’t mutate back to a virulent form and don’t require refrigeration • Downside: these vaccines stimulate a weaker immune response and may require several additional doses (or “booster shots”)
Killed (inactivated) vaccines Attributes • Immune response • poor; only antibody - no cell immediated immune response. • response is short-lived and multiple doses are needed. • may be enhanced by the incorporation of adjuvants into the vaccine preparation (see below) • 1. Safety • Inactivated, therefore cannot replicate in the host and cause disease. • Local reactions at the site of injection may occur. • 2. Stability • Efficacy of the vaccine does not rely on the viability of the organisms. • These vaccines tend to be able to withstand more adverse storage conditions. • 3. Expense • Expensive to prepare
Killed (inactivated) vaccines When safe live vaccines are not available, either because attenuated strains have not been developed or else because reversion to wild type occurs too readily, it may be possible to use an inactivated preparation of the virulent organism to immunize the host. • The organism is propagated in bulk, in vitro, and inactivated with either beta-propiolactone or formaldehyde. These vaccines are not infectious and are therefore relatively safe. However, they are usually of lower immunogenicity and multiple doses may be needed to induce immunity. In addition, they are usually expensive to prepare. • Subcellular fractions • When protective immunity is known to be directed against only one or two proteins of an organism, it may be possible to use a purified preparation of these proteins as a vaccine. The organism is grown in bulk and inactivated, and then the protein of interest is purified and concentrated from the culture suspension. These vaccines are safe and fewer local reactions occur at the injection site. However, the same disadvantages of poor immunogenicity and the need for multiple boosters applies. • Recombinant proteins • Immunogenic proteins of virulent organisms may be synthesized artificially by introducing the gene coding for the protein into an expression vector, such as E-coli or yeasts. The protein of interest can be extracted from lysates of the expression vector, then concentrated and purified for use as a vaccine. The only example of such a vaccine, in current use, is the hepatitis B vaccine.
Type of Vaccine: Subunit Vaccines • Subunit vaccines dispense with the entire microbe and just use important parts of it: the antigens that stimulate the immune system • The chances of an adverse reaction to the vaccine are lower • Downside: identifying the precise antigens which best stimulate the immune system is difficult and time-consuming • It may be possible to manufacture the antigen molecules using recombinant DNA technology
Subunit Vaccines • Immune response can be stimulated by one or a set of viral proteins. • This was first demonstrated by hepatitis B and influenza vaccines • These can be a lot safer than attenuated or inactivated vaccines • The subunits included are determined by identifying which proteins the antibodies recognize. • Subunits vaccines • Composed solely of purified protein • can be delivered to body by means of a nonpathogenic virus, bacteria, etc
Type of vaccine: Toxoid Vaccines • Toxoid vaccines are used when a bacterial toxin (i.e. a harmful chemical given off by the microbe) is the main cause of the illness • The bacterial toxins are inactivated by treating them with a solution of formaldehyde • These detoxified toxins are called “toxoids” and are safe for use in vaccines • The immune system produces antibodies that lock onto and block the toxin.
Type of Vaccine: Conjugate Vaccines • Sometimes microbes contain an outer coating of polysaccharides that hide the antigens so that younger children’s immune system can’t recognize them • Scientists overcome this obstacle by linking antigens that a child can respond to to the polysaccharides • That way, the child’s immune system will become trained to respond to the foreign polysaccharides
Type of vaccine: DNA Vaccines • DNA vaccines would use the naked DNA from a few genes of the invading organism • Those genes would be introduced into the body, taken up by some of the cells • Those host cells would then produce the antigens molecules, allowing them to be displayed and stimulating the immune system • The host’s own cells would become the vaccine-making factory • Still experimental, but being tested against malaria, influenza, herpes, and HIV • In another version, called a “vector vaccine” the DNA is ferried into the host cells by harmless viruses
Type of Vaccine: Combination Vaccine • Several vaccines are combined into one dose • DTP = diphtheria, tetanus, pertussis • MMR = measles, mumps, rebella
Adjuvants Certain substances, when administered simultaneously with a specific antigen, will enhance the immune response to that antigen. Such compounds are routinely included in inactivated or purified antigen vaccines. Adjuvants in common use: • Aluminium salts • First safe and effective compound to be used in human vaccines. • It promotes a good antibody response, but poor cell mediated immunity. • Form precipitate with antigen, making complex more antigenic 2. Liposomes and Immunostimulating complexes (ISCOMS) 3. Complete Freunds adjuvant is an emulsion of Mycobacteria, oil and water • Too toxic for man • Induces a good cell mediated immune response. 4. Incomplete Freund's adjuvant as above, but without Mycobacteria. 5. Muramyl di-peptide • Derived from Mycobacterial cell wall. 6. Cytokines • IL-2, IL-12 and Interferon-gamma. • Possible modes of action: • By trapping antigen in the tissues, thus allowing maximal exposure to dendritic cells and specific T and B lymphocytes. • By activating antigen-presenting cells to secrete cytokines that enhance the recruitment of antigen-specific T and B cells to the site of inoculation.
Timeline of Vaccines • 18th century • 1796 First vaccine for smallpox, first vaccine for any disease • 19th century • 1882 First vaccine for rabies • 20th century • 1932 First vaccine for yellow fever • 1945 First vaccine for influenza • 1952 First vaccine for polio • 1954 First vaccine for Japanese encephalitis • 1957 First vaccine for adenovirus-4 and 7 • 1962 First oral polio vaccine • 1964 First vaccine for measles • 1967 First vaccine for mumps • 1970 First vaccine for rubella • 1974 First vaccine for chicken pox • 1977 First vaccine for pneumonia • 1978 First vaccine for meningitis • 1981 First vaccine for hepatitis B • 1992 First vaccine for hepatitis A • 1998 First vaccine for rotavirus
DNA Vaccines • DNA vaccines are at present experimental, but hold promise for future therapy since they will evoke both humoral and cell-mediated immunity, without the dangers associated with live virus vaccines. • The gene for an antigenic determinant of a pathogenic organism is inserted into a plasmid. This genetically engineered plasmid comprises the DNA vaccine which is then injected into the host. Within the host cells, the foreign gene can be expressed (transcribed and translated) from the plasmid DNA, and if sufficient amounts of the foreign protein are produced, they will elicit an immune response. • in recent years a new type of vaccine, created from an infectious agent's DNA called DNA vaccination, has been developed. It works by insertion (and expression, triggering immune system recognition) into human or animal cells, of viral or bacterial DNA. These cells then develop immunity against an infectious agent, without the effects other parts of a weakened agent's DNA might have. As of 2006, DNA vaccination is still experimental, but shows some promising results.
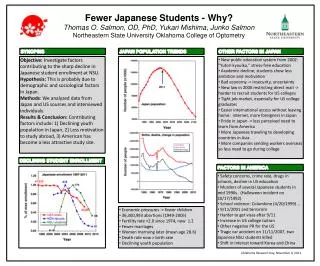
Vaccines in General Use Measles • Live attenuated virus grown in chick embryo fibroblasts, first introduced in the 1960's. Its extensive use has led to the virtual eradication of measles in the first world. In developed countries, the vaccine is administered to all children in the second year of life (at about 15 months). However, in developing countries, where measles is still widespread, children tend to become infected early (in the first year), which frequently results in severe disease. It is therefore important to administer the vaccine as early as possible (between six months and a year). If the vaccine is administered too early, however, there is a poor take rate due to the interference by maternal antibody. For this reason, when vaccine is administered before the age of one year, a booster dose is recommended at 15 months.
Measles—UnitedStates, 1950-2002 Vaccine Licensed
Vaccines in General Use Mumps • Live attenuated virus developed in the 1960's. In first world countries it is administered together with measles and rubella at 15 months in the MMR vaccine. • The current "Jeryl Lynn" strain of the mumps vaccine was developed by Dr. Maurice Hillman from the mumps virus that infected his 5-year-old daughter (whose name was Jeryl Lynn). This vaccine, combined with rubella or both rubella and measles vaccines (MMR), has been widely used worldwide (300 million doses given) since it was approved by the FDA in 1967.
Vaccines in General Use Polio • Two highly effective vaccines containing all 3 strains of poliovirus are in general use: • The killed virus vaccine (Salk, 1954) is used mainly in Sweden, Finland, Holland and Iceland. • The live attenuated oral polio vaccine (Sabin, 1957) has been adopted in most parts of the world; its chief advantages being: low cost, the fact that it induces mucosal immunity and the possibility that, in poorly immunized communities, vaccine strains might replace circulating wild strains and improve herd immunity. Against this is the risk of reversion to virulence (especially of types 2 and 3) and the fact that the vaccine is sensitive to storage under adverse conditions. - Orimune® • The inactivated Salk vaccine is recommended for children who are immunosuppressed. • 3 types of live polio virus, magnesium chloride, amino acid, polysorbate 80, purified water, neomycin, sulphate, streptomycin, penicillin and monkey kidney cell cultures.
Inactivated vaccine Live oral vaccine Last indigenous case Poliomyelitis—United States, 1950-2002
Vaccines in General Use Rubella • Live attenuated virus. Rubella causes a mild febrile illness in children, but if infection occurs during pregnancy, the fetus may develop severe congenital abnormalities. Two vaccination policies have been adopted in the first world. In the USA, the vaccine is administered to all children in their second year of life (in an attempt to eradicate infection), while in Britain, until recently, only post pubertal girls were vaccinated. It was feared that if the prevalence of rubella in the community fell, then infection in the unimmunized might occur later - thus increasing the likelihood of infection occurring in the child-bearing years. This programme has since been abandoned in Britain and immunization of all children is the current practice. • MMR — live measles virus, live mumps virus, live rubella virus, chick embryo, human foetal cells, neomycin, sorbitol, gelatine.
Vaccines in General Use Rabies • No safe attenuated strain of rabies virus has yet been developed for humans. Vaccines in current use include: • The neurotissue vaccine - here the virus is grown in the spinal cords of rabbits, and then inactivated with beta-propiolactone. There is a high incidence of neurological complications following administration of this vaccine due to a hypersensitivity reaction to the myelin in the preparation and largely it has been replaced by • A human diploid cell culture-derived vaccine (also inactivated) which is much safer. There are two situations where vaccine is given:a) Post-exposure prophylaxis, following the bite of a rabid animal:A course of 5-6 intramuscular injections, starting on the day of exposure. Hyperimmune rabies globulin may also administered on the day of exposure. • b) Pre-exposure prophylaxis is used for protection of those whose occupation puts them at risk of infection with rabies; for example, vets, abbatoir and laboratory workers. This schedule is 2 doses one month apart ,and a booster dose one year later. (Further boosters every 2-3 years should be given if risk of exposure continues).