Download
1 / 26
270 likes | 470 Views
Objective Measurement of Adequacy of Vascular Anastomosis in Renal Transplant. Dr Ajay Aspari Raghunath Dr Dilip C Dhanpal Department of Nephro -Urology and Transplantation Sagar Hospitals, Jayanagar Bangalore. Introduction. Problems with Inadequate Vascular Anastomosis

E N D
Objective Measurement of Adequacy of Vascular Anastomosis in Renal Transplant Dr Ajay AspariRaghunath Dr Dilip C Dhanpal Department of Nephro-Urology and Transplantation Sagar Hospitals, Jayanagar Bangalore
Introduction • Problems with Inadequate Vascular Anastomosis • Thrombotic complications • Renal Artery Thrombosis • Stenotic Complications • Renal Artery Stenosis • Haemorrhagic Complications AFFECTING GRAFT AND PATIENT SURVIVAL Osmany , Shokeir A , Ali-el Dein B et al [2003]Vascular Complications After Live Donor Renal Transplantation: Study of Risk Factors And Effects on Graft and Patient survival. Journal of Urology 169, 859–862
Introduction contd. • Criteria for assessment of Adequacy of Vascular Anastomosis in Renal transplant • Subjective Criteria • Thrill • Pulsations • Surrogate Criteria • Colour of Kidney • Turgidity of Kidney • Immediate urine output via transplanted kidney NO OBJECTIVE CRITERION FOR A GOOD ANASTOMOSIS INTRAOPERATIVELY
1 2 3 4
If the above are NOT satisfied, • Systemic Measures • Central Venous Pressure • Blood Pressure • Local Measures • Intra arterial Papaverine • PeriarterialLignocaine spray • On table USG Doppler • Biopsy of Kidney [ in case of suspected rejection ] • A redo anastomosis is in order if the above are not satisfactory .John M Barry, Transplantation as Treatment of End-Stage Renal Disease and Technical Aspects of Renal transplantation
Aim • To define an objective measurement of Vascular Anastomotic adequacy • Pilot study • First ever Objective Criteria to be described
Materials and Methods • Recruitment • Every consecutive patient undergoing transplant • End to End anastomosis [Internal Iliac A. to Tx Renal A. ] • Exclusion • Pediatric • End to side [External Iliac A. To Tx Renal A.] • Thromboendarterectomy [ 1 case ] • 22G Cannula for intra arterial pressure • Why 22 Gauge ?? • Measurement across anastomosis • Technique • Study period – January 2011 to Date
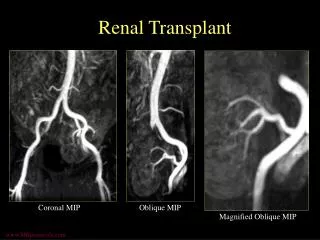
Follow up • USG Doppler studies • Post Operative Day -1 • Evaluation of Renal Blood flow • From Renal artery uptoArcuate arteries
Resistive Index Criteria • Main Renal Artery • Divisional Artery • Anterior • Posterior • Segmental Artery • Interlobar Artery • Lobular Artery • Arcuate Artery
Resistive Index Criteria • Tool for assessing changes in renal perfusion Line H , Naesens M , Lerut E et al [2013] Intrarenal Resistive Index after Renal Transplantation. New England Journal of Medicine. 369:1797-1806 M Darnel, D Schnell, F Zeni [2010] Doppler-Based Renal Resistive Index: A Comprehensive Review.Yearbook of Intensive Care and Emergency Medicine. pp 331-338
Resistive Index Criteria • Accepted RI Criteria – • 0.6 – 0.8 Line H , Naesens M , Lerut E et al [2013] Intrarenal Resistive Index after Renal Transplantation. New England Journal of Medicine. 369:1797-1806
Resistive Index • Pulsatility index • [ Systolic Velocity – Diastolic Velocity] / Mean Velocity
Results • 13 cases • Least gradient = 6 mm Hg • Highest Gradient = 17 mm Hg • Mean Pressure gradient = 10.76 mmHg • Median Pressure Gradient = 9 mm Hg • Mode = 12 mm Hg
Correlation Coefficients • Pressure gradient vs Resistive index Hilar r = 0.9 Segmental Arteries r = 0.81 ArcuateArteries r = 0.85
Discussion • Correlation between Pressure gradient and Vascular resistive index • Higher the gradient, higher the resistance • Utility of pressure gradient
Discussion • Why not Doppler On Table?? • Doppler may pick up readings only for stenosis beyond 60-70% • Not reflective of mild to moderate stenosis • Doppler studies are no longer done to diagnose Renal Artery Stenosis
Discussion • Such a technique has been recommended for Lung transplant • Has been carried out in Coronary artery surgeries • > 30mm Hg is unacceptable warranting a redo anastomosis • No literature for Renal transplant • Since Renal Vessels are bigger than Coronary vessels, we arbitrarily propose a cut off of 20 mmHg Siddiqui A ,Bose A K, Ozalp F et al [2013] Vascular anastomotic complications in lung transplantation: a single institution’s experience. Interactive CardioVascular and Thoracic Surgery 17 - 625–631
Discussion • To define the Criterion based on Pressure Gradient • Require further studies and also animal experiments
Conclusion • Simple method for measurement of Vascular Adequacy • Application of Pressure gradient measurement will reflect: • Lesser rates of failed transplant • Criterion useful for Young Transplant surgeons • Eg. at high volume centres and teaching institutes where in inadequate anastomosis on table is quickly detected and a redo is done rather than flogging a tired horse
References • Osmany, ShokeirA , Ali-el DeinB et al [2003]Vascular Complications After Live Donor Renal Transplantation: Study of Risk Factors And Effects on Graft and Patient survival. Journal of Urology 169, 859–862 • John M Barry, Transplantation as Treatment of End-Stage Renal Disease and Technical Aspects of Renal Transplantation • Line H , Naesens M , Lerut E et al [2013] Intrarenal Resistive Index after Renal Transplantation. New England Journal of Medicine. 369:1797-1806 • M Darnel, D Schnell, F Zeni [2010] Doppler-Based Renal Resistive Index: A Comprehensive Review.Yearbook of Intensive Care and Emergency Medicine. pp 331-338 • Siddiqui A ,Bose A K, Ozalp F et al [2013] Vascular anastomotic complications in lung transplantation: a single institution’s experience. Interactive CardioVascular and Thoracic Surgery 17 - 625–631