Download
1 / 75
760 likes | 810 Views
Learn about acoustic neuroma, also known as vestibular schwannoma, its symptoms, classifications, staging, symptoms, management, surgical approaches, and proton stereotactic radiotherapy.

E N D
Acoustic Neuroma & Glomus Tympanicum Dr. Vishal Sharma
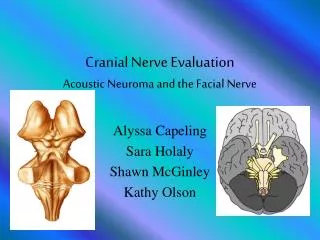
Introduction A.K.A.:vestibular schwannoma / neurilemmoma Benign, encapsulated, slow growing tumour arising from Schwann cells of superior vestibular division of 8th nerve within internal auditory canal Rarely from inferior vestibular or cochlear division
Tumour growth Tumor expansion within internal auditory canal causes widening & erosion of I.A.C. appears in cerebello-pontine angle (> 2.5 cm) involves 5th, 7th, 9th, 10th, 11th cranial nerves displacement of brainstem & cerebellum raised intracranial pressure Involvement of 6th & 3rdcranial nerves
Classificationas per size 1. Intra-canalicular: confined to I.A.C. 2. Small: up to 1.5 cm 3. Medium: 1.5 to 4 cm 4. Large: over 4 cm
Epidemiology • 10% of all brain tumors • 80% of all Cerebello-pontine angle tumors • Age: 40-60 yrs • Male : Female = 3:2 • Unilateral (90%); Bilateral (10%) • Bilateral = von Recklinghausen’s neurofibromatosis
Clinical Staging • Otological stage: due to pressure on 8th nerve • Other Cranial nerve involvement • Brainstem + Cerebellar involvement • Raised intra-cranial tension • Terminal stage: failure of vital centers of brainstem & cerebellar tonsil herniation
Otological symptoms & signs • Progressive, unilateral sensorineural deafness • Poor speech discrimination (disproportionate) • Tinnitus • Mild vertigo • Nystagmus Vestibular symptoms appear late due to slow tumor growth & vestibular compensation
Other Cranial nerve palsy Trigeminal: first nerve to be involved • Loss of corneal reflex • Pain, numbness and paresthesia of the face Facial: • Hypoaesthesia of posterior external auditory canal wall (Hitselberger’s sign) • Facial weakness, Loss of taste, ed lacrimation
Other Cranial nerve palsy Glossopharyngeal, Vagus & Accessory Spinal: • Dysphagia • Hoarseness • Nasal regurgitation • Decreased gag reflex Abducent & Oculomotor: • Diplopia
Brainstem involvement Ataxia Weakness of arms & legs Tendon reflexes exaggerated Cerebellar involvement Ataxic gait (fall on affected side) Intention tremors Past-pointing Dysdiadochokinesia Increased Intra-cranial tension Headache Projectile vomiting Blurred vision Papillodema Abducent nerve palsy
First Symptoms Hearing loss: 80-100 % Vertigo: 10-50 % Tinnitus: 5-10 % Ear ache: 5 % Sudden hearing loss: 5% Facial paralysis: 1-2 %
Investigations • Pure Tone Audiometry:high frequency SNHL • Speech audiometry:SD scores < 30% • Tone decay test:positive • Stapedial Reflex: Decay > 50 % in 10 sec • B.E.R.A.:wave V >4.2 ms; inter-wave V >0.2 ms • Caloric test:I/L canal paresis or no response • C.T. scan with contrast: for tumor > 0.5 cm • M.R.I. with gadolinium contrast:best
Speech Audiometry Roll over phenomenon
Treatment 1. Observation 2. Microsurgical removal: (partial or total) • Trans-labyrinthine approach • Retro-sigmoid or Sub-occipital approach • Middle Cranial Fossa approach • Combined approach 3. Proton Stereotactic Radiotherapy 4. Brainstem Implant: after B/L tumor excision
Observation Indications: • Age > 60 years with small tumor & no symptoms • Tumour in only hearing / better hearing ear Serial MRI used to follow growth pattern. Treatment recommended if hearing is lost or tumor size becomes life threatening.
Incisions Middle cranial fossa Retro-sigmoid Trans-labyrinthine
Surgical Approach Protocol 1. Intra-canalicular: Middle cranial fossa approach 2. Small (<1.5 cm): Retrosigmoid approach 3. Medium (1.5 - 4 cm) a. Hearing fine**: Retrosigmoid approach b. Hearing bad:Trans-labyrinthine approach 4. Large (>4 cm): Trans-labyrinthine/ Combined **Pure Tone Average < 30 dB, S.D. Score >70%
Proton stereotactic radiotherapy Single high dose of radiation delivered on a small area to arrest or kill tumor cells. Minimal injury to surrounding nerves & brain tissue Gamma Knife: radioactive cobalt LINAC X-knife: linear accelerator Cyber-Knife: robotic radio-surgery system Indication: 1. Surgery refused / contraindicated 2. Post-operative residual tumour
Synonym: Chemodectoma Non-chromaffin paraganglioma Commonest benign tumour of middle ear derived from glomus bodies distributed along parasympathetic nerves of head & neck Consists of paraganglionic cells derived from embryonic neuroepithelium Introduction
Introduction Histologically benign but locally invasive, highly vascular, non-encapsulated, slow growing tumors 10 % tumors: familial 10 % tumors: multicentric 10 % tumors: functional (secrete catecholamines) 4 % tumors: metastatic
Histopathology Typical cellular groups ("Zellballen") surrounded by a capillary network
Types Glomus jugulare Arises along jugular bulb & superior vagal Ganglion, near floor of middle ear Glomus tympanicum Arises along tympanic plexus on promontory formed by tympanic branch of Glossopharyngeal nerve, near medial wall of middle ear