Download
1 / 89
900 likes | 942 Views
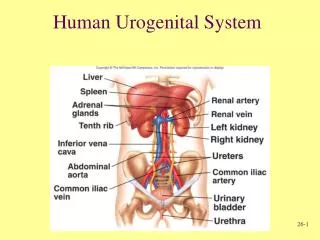
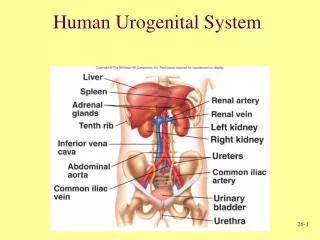
UROGENITAL SYSTEM. Kidney & Ureter PREPARED BY DR. PANCHAJANI.R. Kidney. ANATOMY Situated retroperitonially in the posterior abdominal wall one on each side of vertebral column. Extends from upper border of T12 to the centre of the body of L3 vertebra.

E N D
UROGENITAL SYSTEM Kidney & Ureter PREPARED BY DR. PANCHAJANI.R
Kidney ANATOMY • Situated retroperitonially in the posterior abdominal wall one on each side of vertebral column. • Extends from upper border of T12 to the centre of the body of L3 vertebra. • 11 cm long ,6cm broad,3cm thick, lateral border convex, medial border concave with a hylum. • Structures in hylum – renal artery ,renal vein, renal pelvis. • upper pole –suprarenal gland, • lower pole- 1inch above iliac crest • Capacity of renal pelvis- 10ml
Kidney • Renal angle- angle between the 12thrib & outer border of sacrospinalis. Pressure over this point elicits pain in kidney lesions. • Hepato renal pouch- related to upper pole of kidney. collection of extravasated fluid in this pouch following liver& biliary tract surgeries. • Outer brownish cortex , inner pale medulla • Pelvis divides 2-3 major calyces which then divides in to 7-13 minor calyces. • Each kidney – 1-3 million Uriniferous tubules, each has a Collecting part(Collecting tubule) & Secretory part( Nephrones )
Kidney • Blood supply- Renal artery arises from abdominal aorta.(between L1-L2) • 95% of abdominal aneurism arises below the level of origin of Renal artery. • Nerve supply- T10, 11,12 • Lymphatic drainage- Para-aortic nodes.
URETER • 25- 30 cm long,3-4mm in diameter. • Begins with in the renal sinus as a funnel -shaped dilatation called renal pelvis. It open at the lateral wall of the trigone of the urinary bladder. Not attached to any fixed structures. so easily displaced or obstructed • In females uterine artery crosses the ureter about 2cm lateral to the cervix. (important in hysterectomy) • Normal sites of constrictions - PUJ, At the brim of lesser pelvis, Along its passage through the bladder wall. • Arterial supply – upper- branches of renal & adrenal arteries, middle- branches of arteries of posterior abdominal wall. Lower(pelvic part) - branches of internal iliac arteries • The mean size of ureters on obstructed side was 7mm, stones less than or about 5mm in size can pass through the urinary tract on their own.
INVESTIGATIONS • Blood – RFT- urea, creatinine, BUN, • Urine - microscopic, macroscopic, cytological, bacteriological,biochemical • Plain X-ray-- KUB • Taken in supine position which cover pubic symphysis & lower 2 ribs • Bony parts looked any abnormality • Kidney shadow- visualized in plain x-ray KUB due to difference in the density between kidney (high vascularity) & perinephric fat(low vascularity). • Findings noted are size, location, calcification & stones. • Perinephricfat is absent in children so kidney shadows are not visualized. • Psoas shadow visualised in normal KUB. Obliterated in enlarged kidney, TB spine, psoasabscess, scoliosis, Ca, splenic injury. • Uretericline– looked for any radio opaque shadow( ureteric stone ) • Any lesion in bladder, prostate, urethral areas.
Investigations 4. Intra venous urogram (IVU/IVP) • Renal fuction must be normal • Hydronephrosis - clubbing of calyces • Hoarse shoe kidney - flower vase appearance • Ureterocele - cobra head appearance • Poly cystic kidney - spider leg appearance • RCC - irregular filling defect, spider leg • To see functions of kidney in stones , obstructions.
Investigations 3. Retrograde pylography(RGP) Urinary TB, Urothelialtumours 4. Renal angiogram Indications • Renal artery stenosis, RA atheroma, RA aneurysm ,RCC • Arterial anomalies 5. Micturatingcystourethrography (MCU) Indications • Vescicoureteric reflux • Posterior urethral valves 6. Ascending urethrogram • Stricture urethra • USG- High resolution for size, thickness, obstructions • Trans rectal USG- for Ca prostate • CT, MRI, Isotope Renography, Cystoscopy
HAEMATURIA Gross – visible Microscopic-More than 5RBC ‘S/ HPF • Early(initial) H – urethral origin distal to external sphincter • Terminal H - Bladder neck or prostate origin • Diffuse(total) – in the bladder or upper urinary tract • False H - Discolouration of urine from pigments such as food colouring and myoglobin • Silent H - Tumour of kidney or bladder
Haematuria – causes • Renal injury • Urinary stones • Wilm’stumour • TB • RCC • Cystitis • Bladder tumour • Urinary bilharziasis • BPH, Ca prostrate • Renal infart • Glomerulonephritis • Blood dyscrasias
Haematuria – investigations • Urine R/E, C&S • USG- Stones, tumours • Cystourethroscopy- for bladder& urethral pathology • IVU- for functions of kidney • Urinary cytology- for malignancy • BT, CT, PT, Platelet count • CT abdomen • RFT Management- cause should be identified & treated
Hoarse shoe kidney • fusion of lower pole common • common site -in front of the 4th lumbar vertibrae • Mass in the mid line of 4th lumbar vertebrae • IVU – medialisation of lower calyces & curving of ureter like a flower vase
Poly cystic kidney • Bilateral • Occurs at the junction of distal tubule and the collecting duct • Renal mass moves with respiration, ballotable, movable • 75% - hypertension, 25% haematuria • IVU- Spider leg pattern with an elongated compressed renal pelvis,narrowed & stretched calyces.
Retrocavalureter • Developmental defect of IVC, right ureter passes behind the IVC, right hydronephrosis with hydroureter. • IVU- Hydronephrosis with reverse J sign • Treatment( Tt) - Anderson Hynes operation
URETEROCELE • Cystic enlargement of the intra mural portion of ureter due to congenital atresia of the ureteric orifice. • IVU- Adder head or cobra head appearance. • Cystoscopy– transluscent thin walled cyst surrounding the ureteric orifice • Tt. - Cystoscopicuretericmeatotomy.
Renal injuries • Associated with Blunt injury abdomen • It is extraperitoneal Types- • small & large subcapsular • Cortical laceration • Laceration with haematoma • Medullarylaceration with bleeding in to pelvis • Cortico- medullary complete laceration • Hilarinjury – most dangerous
Renal injuries Clinical features • Features of Shock • Haematuria, sometimes delayed profuse haemorrhage ( haematuria between 3rd day & 3rd week), clot colic • Swelling & tenderness in loin. • Paralytic ileus with abdominal distension
Renal injuries Investigations • CT Scan - Grading of injury, Associated injuries, functions of kidney. • USG Abdomen - site& type of injury., haemoperitoneum, associated injuries, effect of therapy by repeating it. • IVU - Functions of injured& normal Kidney , • RFT - Blood Urea, Creatinine, electrolytes, haematocrit, blood Grouping. • Other - Chest X-ray, CT, plain X-ray abdomen .
Renal injuries Treatment • Conservative - catheterization, blood transfusion, monitor vital signs, urea, creatinine etc.. • Surgical- indications- blood loss, haematoma, hilar injury • 10- 20 % cases -Gentle suturing, Nephrostomy, Nephrectomy
RENAL TUBERCULOSIS • Secondary to pulmonary TB, Bacilli causes lesions in the renal cortex & it spreads along the ureter causing tubercular ureteritis & stricture ureter. Pathology • Through blood it reaches the glomeruli causing caseatinggranuloma with Langerhan’stype of giant cells & epitheloid cells. These granuloma united to form, • TB papillary ulcer • Cavernous form • Hydronephrosis • Pyonephrosis • perinephric abscess, calcification, casceous kidney, miliary TB, TB cystitis leads to golf hole ureter & thimble bladder,prostatitis, vesciculitis, stricture etc..
RENAL TUBERCULOSIS Clinical features • Common in males, right side, frequency, polyuria, sterile pyuria painful micturition with often haematuria , renal pain, suprapubic pain. • Kidney rarely palpable. Enlarged prostate & seminal vescicles. Acute pyelonephritis. Features of urinary stones, UTI, Dyspareunia , menstrual irregularities. Fever& weight loss, cough, expectoration, haemoptysis.
RENAL TUBERCULOSIS Investigations • Hb% & ESR increased • Mantoux test positive. • Chest X- ray • Three consecutive early morning urine is sent for microscopy & culture • USG • Plain X- ray KUB - shows calcification • CT abdomen& pelvis – see hydronephrosis, shrunken kidney, stricture, necrosis • IVU – Hydrocalyx, narrowing of calyx, stricture ureter • RGP- is useful, ureter, pelvis, calyces seen, sampling of urine taken • CYSTOSCOPY- multiple tubercles, bladder spasm, oedema of uretericorifice forming golf hole ureter • MCU- to see ureteric stricture , reflux
RENAL TUBERCULOSIS Treatment • Anti TB treatment • Hydronephrosis - anderson’spyeloplasty • TB abscess- drainage • Ureteral stricture – Stenting/ Reimplantation of the ureter in to bladder • Thimble bladder - hydraulic dilatation/ ileocystoplasty/ caecocystoplasty/ sigmoid colocystoplasty • In unilateral lesion with gross impairement of renal function- nephroureterectomy
Hydronephrosis • It is an aseptic dilatation of whole or a part of pelvi-calyceal system of kidney due to partial or intermittent obstruction to the out flow of urine. • Hydronephrosis refers to dilatation of renal pelvis and calyces with accompanying atrophy of the parenchyma. • Cause by obstruction to the outflow of urine
Hydronephrosis – obstruction levels • Renal pelvis • Pelviureteric junction • Ureter • Bladder • Urethra
Hydronephrosis – causes • Aetiology ; it can be unilateral/ bilateral Unilateral • Extramural- • Aberrant renal vessels( vein/ artery)compressing the ureter - common on left side • Compression by a growth/ Tumour- Ca cervix, Ca rectum, prostrate, colon etc.. • Retroperitoneal fibrosis • Retrocavalureter
Hydronephrosis – unilateral causes Intramural • Congenital PUJ obstruction • Ureterocele • Inflammatory stricture • Ca ureter • Narrow ureteric orifice • Stricture ureter (following removal of stones, pelvic surgeries, TB ureter) Intra luminal • Stone in the renal pelvis or ureter • Sloughed papilla in papillary necrosis
Hydronephrosis – Bilateral causes Bilateral • Congenital- stricture of external urethral meatus, pinhole meatus Congenital posterior urethral valve, urethral atresia. • Acquired - BPH Ca prostate Post operative bladder neck scarring Inflammatory / traumatic urethral stricture Phimosis Ca cervix involving both ureters Bladder Ca • Congenital PUJ obstruction is the most common cause of HN • Often it is bilateral & presentation on one side is earlier than the other side. • Aberrant renal artery or vein in the lower pole can compress PUJ causing HN. Renal angiogram confirms the diagnosis.
Pathophysiology • Due to aetiological factors obstruction of the urine flow fluid backs up in to the kidney causing dilatation of renal pelviscausingbarotrauma/ pressure trauma higher pressure causes irreversible destruction of the nephrones hypertrophy of the kidney as a consequence of increased work load hydronephrosis renal failure
Pathology • Changes depends on whether the kidney has an extrarenal or intra renal pelvis- commonly extra renal • In extra renal pelvis first the pelvis alone become dilated , at time goes on if the obstruction is not relieved calyces become dilated& renal parenchyma is progressively destroyed by pressure atrophy • In a kidney with intra renal pelvis destruction of parenchyma occurs rapidly
Pathology • Kidney is massively enlarged with greatly distended pelvicalyceal system. • The renal parenchyma is compressed and atrophied with obliteration of the papilla and flattening of the pyramids. • Pressure changes on the pelvis later calyces & renal parenchyma. • Gradually parenchyma thins out due to destruction & it dilates& affects secretory function • Parenchymal thickness of less than 2 mm is unlikely to function .In bilateral cases such patients will go for renal failure. • Depending on obstruction one or both ureter may also dilated( hydroureter)
Symptoms & signs of HN • Male: female- 2: 1 • Right side is more common • Asymptomatic in some conditions • Dull aching loin pain with dragging sensation or heaviness (Pain is felt in the renal area.) worse by excessive fluid intake • Haematuria • Anuria/ oliguria • Urinary infection, dysuria, frequency • Calculi • Azotemia – abnormaly high level of nitrogen containing compounds( urea, creatinine etc..) in blood • Unexplained vague GIT symptoms • Some large hydronephrosis can be palpable( mass in the loin which is mobile, ballotable, moves with respiration with dullness in renal angle). • Dietl’s crisis- after an acute attack of renal colic , swelling in the loin is seen which disappears after passing large volume of urine. • Occassionally hypertension. • Distension of bladder if urethra is obstructed.
Clinical course • Bilateral complete obstruction produce anuria which need soon medical attention. • Incomplete bilateral obstruction produce polyuria rather than oliguria as a result of defect in tubular concentrating mechanism
Clinical course • Unilateral hydronephrosis may be silent for long period unless other kidney is affected • Bilateral hydronephrosis usually lead to uremia • Early removal of obstruction can return the kidney function • However with the time the changes become irreversible
INVESTIGATIONS - HN • RFT- urea, creatinine • Urine microscopy • USG • IVU • CT • Isotope renography- DTPA scan-pentetic acid • Complications- pyonephrosis, perinephric abscess, renal failure in bilateral cases
Treatment -secondary to cause • Stones- pyelolithotomy/ ureterolithotomy • Stricture – stricturoplasty or excision and end to end anastamosis • Aberrant vessel- transection of the ureter and anastomosis in front of the vessel. • BPH- TURP • Ca prostrate- TURP+ Hormonal therapy • Urethral stricture- urethroplasty • Meatal stenosis- meatoplasty • Phimosis – circumcision
Management of congenital hydronephrosis • Patients with congenital PUJ dysfunction presents congenital hydronephrosis • Congenital hydronephrosis can be defined as more than 10mm antero-posterior diameter of renal pelvis at 20 weeks of gestation. • Management differs according to the grades of hydronephrosis, which is based on renal pelvic diameter.
MANAGEMENT • Grading- mild -11-20mm • Moderate-21- 35mm • Severe- > 35mm • Mild case is managed conservatively with serial monitoring of pelvic diameter by USG and of renal function. • Moderate is also managed by serial monitoring. Any deterioration of renal function is an indication for surgical intervension • Severe HN should be treated early Anderson – Hynes pyeloplasty to prevent permanent damage to kidney.
Anderson Hynes Pyeloplasty • In this operation , the upper third of the ureter and the renal pelvis are mobilised. • Anastomosis is made between ureteric end and kidney. • A nephrostomy tube is passed , which serves to protect the anastomosis
Pyonephrosis • Collection of pus in the pelvicalyceal system (a multi loculated cyst). Causes – • Infection of hydronephrosis • Following acute pyelonephritis • Complication of renal calculi( stone in renal pelvis or stag horn calculi) Clinical features- usually unilateral • Triad – anemia, fever, loin swelling • Tender mass in loin, smooth, soft, not mobile , not move with resp. • Cystitis, pyuria, burning micturition. • Fever, chill, rigor
Pyonephrosis Investigations • Plain X-ray KUB – For Renal calculi • IVU- For HN • Cystoscopy – cystitis • USG • DTPA Scan Treatment – medicinal treatment • Drainage- through loin incision & nephrostomy tube • Kidney is totally destructed- sub capsular nephrectomy • In Bilateral- bilateral nephrostomy with J stending to keep ureter patent
RENAL CARBUNCLE • A localised inflammatory necrotic mass of tissue involving renal parenchyma. • Causative organism- staphylococcus aureus & coliforms. • Source- cutaneous infection like boil & carbuncle. • Presents as ill-defined tender swelling in the loin, with pyrexia, leucocytosis. • Staphylococci can be isolated from the urine. • IVU- obliteration of group of calyces like RCC • Treatment- Drainage with malecots catheter • Severe cases- Nephrectomy
PERINEPHRIC ABSCESS Causes • Infection of a perinephrichaematoma • Perforation of renal abscess or carbuncle • TB perinephric abscess • Extension of cortical abscess • Haematogenous spread • Extension of appendicular abscess • Periureteral lymphatic spread C/F- high fever, fullness in the loin, tenderness and rigidity, scoliosis with concavity towards the side of abscess.
PERINEPHRIC ABSCESS Investigations- TC elevated • X- ray KUB- obliteration of psoas shadow, scoliosis, elevation of hemi diaphragm. • IVU- 2 films- lying down & erect position. Normally in erect posture downward displacement of kidney is seen. It is not seen in perinephric abscess- Mathe’s sign. • USG • CT Scan is diagnostic Treatment- medicinal • Under G/A drainage through lumbar incision , pus sent for C/S