Download
1 / 52

E N D
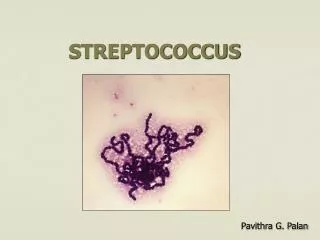
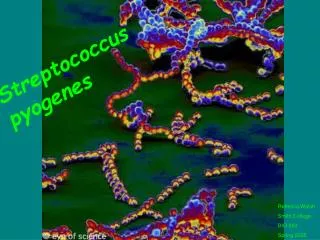
STREPTOCOCCUSPneumoniae Dr.T.V.Rao MD Dr.T.V.Rao MD
Microbial Diseases of the Upper Respiratory System Laryngitis: S. pneumoniae, S. pyogenes, viruses Tonsillitis: S. pneumoniae, S. pyogenes, viruses Sinusitis: Bacteria Epiglottitis: H. influenzae Dr.T.V.Rao MD
History • In 1881, the organism, discovered by Leo Escolar, then known as the pneumococcus for its role as an etiologic agent of pneumonia, was first isolated simultaneously and independently by the U.S Army physician George Sternberg and the French chemist Louis Pasteur. Dr.T.V.Rao MD
Pneumococcal disease:a major health threat • Streptococcus pneumoniae is the leading bacterial cause of infection worldwide: - asymptomatic colonisation - common infections (otitis media, …) - life-threating infections (sepsis, meningitis, …) • Despite the introduction of antimicrobial drugs over the past few decades it remains a significant threat to health Dr.T.V.Rao MD
S. pneumoniae • leading cause of pneumonia • particularly young and old • after damage to upper respiratory tract *e.g. following viral infection • bacteremia • meningitis • middle ear infections (otitis media) Dr.T.V.Rao MD
DISEASES CAUSED BY STREPTOCOCCUS PNEUMONIAE PNEUMOCOCCAL INFECTION • Invasive disease • Bacteraemia (blood) • Meningitis (CNS) • Endocarditis (heart) • Peritonitis (body cavity) • Septic arthritis (bones and joints) • Others (appendicitis, salpingitis, soft-tissue infections) • Non-invasive disease • Sinusitis (sinuses) • Otitis media (middle ear) • Pneumonia (lungs) Musher, in Principles and Practice of Infectious Diseases, 1995 Dr.T.V.Rao MD
Streptococcus pneumoniae • Most common cause of both pneumonia overall and fatal pneumonia. • Antibiotic resistance has developed worldwide and is most frequent in pneumococcal serotypes that are most prevalent in children (types/groups 6, 14, 19, and 23). • The incidence of pneumococcal disease is the highest in children < 2 years of age and in adults > 65 years of age. Dr.T.V.Rao MD
Streptococcus pneumoniae • Streptococcus pneumoniae are Gram-positive, lancet-shaped cocci (elongated cocci with a slightly pointed outer curvature). Usually, they are seen as pairs of cocci (diplococci), but they may also occur singly and in short chains. When cultured on blood agar, they are alpha hemolytic Dr.T.V.Rao MD
Streptococcus pneumoniae • Individual cells are between 0.5 and 1.25 micrometers in diameter. They do not form spores, and they are nonmotile. Like other streptococci, they lack catalase and ferment glucose to lactic acid Dr.T.V.Rao MD
Streptococcus pneumoniae • leading cause pneumonia • particularly young and old • after damage to upper respiratory tract • *e.g. following viral infection • bacteremia • meningitis • middle ear infections (otitis media) • capsule: • pneumolysin: • Surface protein adhesinand secretory IgA protease. • Teichoic acid and the Peptidoglycan fragment, phosphorylchorine . S. pneumoniae - diplococci Dr.T.V.Rao MD
PNEUMOCOCCUS: TRANSMISSION AND COLONISATION Fedson, Musher, in Vaccines, 1994 Musher, in Principles and Practice of Infectious Diseases, 1995 Dr.T.V.Rao MD 2.4
PNEUMOCOCCUS: PATHOGENESIS Salyers, Whitt, in Bacterial Pathogenesis, 1994 Dr.T.V.Rao MD
Pneumococcal cell surface Dr.T.V.Rao MD
Antigenic Properties • Type specific capsular polysaccharide • Diffuses culture medium • Specific soluble substance • Classified on Antigenic nature of Capsular polysaccharide • Originally I II III • Heterogeneous group IV ( Classified into 91 types ) Dr.T.V.Rao MD
Typing Done by • 1 Agglutination of cocci with type specific serum • 2. Precepititation of SSS with specific serum • Nuffield 1902 Capsular swelling or quelling reaction • Can be done on the sputum Dr.T.V.Rao MD
Other Antigens • Nucleoprotein inside the cell • Somatic Carbohydrate • Species specific • An Abnormal protein Beta Globulin Dr.T.V.Rao MD
An Abnormal protein Beta Globulin Precipitated with somatic Carbohydrate antigen of Pneumococci • Appears in phase serum of cases of Pneumonia • Disappears during the convalescence • Called C – reactive protein Dr.T.V.Rao MD
C-reactive Protein CRP • Stimulated in Bacterial infection • Inflammation • Malignancies • Tissue destruction • Helpful in Rheumatic fever Diagnosis • Latex Agglutination test Dr.T.V.Rao MD
Toxins in S.pneumoniae • Toxins and other variable factors • oxygen liable hemolysis • Leucocidin • Capsule • Toxin – Pneumolysin x Phagocytosis • Pneumolysin Cytotoxic Cpomplement activation Dr.T.V.Rao MD
The capsule • Composition: polysaccharide • Virulence factor: avoiding phagocytosis • Induce type-specific immune response • More than 90 different serotypes Dr.T.V.Rao MD
Serotyping • The quelling reaction (swelling reaction) forms the basis of serotyping and relies on the swelling of the capsule upon binding of homologous antibody. The test consists of mixing a loopful of colony with equal quantity of specific antiserum and then examining microscopically at 1000X for capsular swelling Dr.T.V.Rao MD
Streptococcus pneumoniae are Alphahemylotic Hemolysis alpha beta gamma Dr.T.V.Rao MD
BIOCHEMICAL REACTIONS • Done in Hiss serum sugars • Bile solubility test positive with 10% sodium deoxycolate • If a drop of solution is put on colony the clearing occurs Dr.T.V.Rao MD
optochin sensitive Not optochin sensitive Bile solubility test Streptex antiserum • Quellung reaction • using antisera • capsule "fixed" • visible microscopically Dr.T.V.Rao MD Latex agglutination - streptococci
Optochin Test ( Ethyl hydrocuperen 1/5,00,000) • The minimum criteria for identification and distinction of pneumococci from other streptococci are bile or optochin sensitivity, Gram-positive staining, and hemolytic activity. Dr.T.V.Rao MD
Not optochin sensitive optochin sensitive Dr.T.V.Rao MD
PNEUMOCOCCAL CARRIER STATE • Disease occurs in persons who are already asymptomatic carriers • Carrier rates 38%-60% in preschool children 29%-35% in school children 9%-25% in junior high school students 18%-29% in adults with children at home 6% in adults with no children at home Virtually all children <2 of age become carriers Dr.T.V.Rao MD
Pathogenesis: the route to infection Colonisation of the respiratory tract Innate and adaptive immune system Replication in the nasopharynx Viral infections, malnutrition mucosal damage Spread to adjacent sites pneumonia middle-ear otitis sinusitis Dr.T.V.Rao MD blood meningitis
Pneumococcus: colonisation and transmission • Exclusively a human pathogen, part of the normal microbial flora of the upper respiratory tract • Transmission: by droplet secretions • Temporalpattern: winter-early spring • Communicability: Unknown. Probably as long as organism in respiratory secretions Dr.T.V.Rao MD
Streptococcus pneumoniae: Symptoms and Signs • Classic description • sudden onset of chills and pleuritic chest pain • followed by fever and then cough productive of rusty sputum. • Varies greatly. • Respiratory tract symptoms may be absent, especially among patients with bacteremic disease. • Lack of fever is not uncommon and indicates a poor prognosis. • Gastrointestinal symptoms such as nausea, vomiting, or diarrhea are present in 15 to 20% Dr.T.V.Rao MD
Types of infection non-invasive • otitis (25-50%) • sinusitis • recurrent bronchitis invasive • pneumonia • sepsis • meningitis Dr.T.V.Rao MD
PNEUMOCOCCAL DISEASE: MENINGITIS • Meningitis • Inflammation of the meninges (membranes surrounding the brain) • Can be caused by a range of microorganisms, as well as be a manifestation of some non-infectious diseases • Pneumococcal meningitis • Invasive pneumococcal disease • Generally, pneumococci invade the CNS from the blood stream • Signs and symptoms1 • Early stages: fever, irritability, neck stiffness, drowsiness • Later stages: headache, seizures, coma • The signs and symptoms are not specific to pneumococcal disease 1 Salyers, Whitt, in Bacterial Pathogenesis, 1994 Dr.T.V.Rao MD
PNEUMOCOCCAL DISEASE: PNEUMONIA major Complication • Bacteraemia in 15-30% of patients with pneumonia • high mortality despite appropriate antibiotic therapy • overall case fatality rate 15-20% for pneumococcal bacteraemia • higher case fatality rates (30-40%) for elderly persons and other vulnerable groups • Spread of pneumococci in the blood to other normally sterile sites can cause other invasive pneumococcal diseases (e.g. meningitis) • Empyema (pus in the pleural cavity) in about 2% of cases 1 Salyers, Whitt, in Bacterial Pathogenesis, 1994 2 Fedson, Musher, in Vaccines, 1994 3 Musher, Clin Infect Dis, 1992 Dr.T.V.Rao MD
Asplenic patients at risk with Pneumococcal Infections • Asplenic patients and those with impaired splenic function are at risk for a fulminant sepsis syndrome usually due to Streptococcus pneumoniae • The combined use of pneumococcal polysaccharide immunization and early administration of oral empiric antibiotic therapy for fever offers a high level of protection against postsplenectomy sepsis Dr.T.V.Rao MD
HIV infection and Pneumococcal Infection • Adults infected with HIV have high rates of invasive pneumococcal disease. • Persons infected with HIV are particularly susceptible to invasive pneumococcal disease, with a 50- to 100-fold higher incidence than the general U.S. population Dr.T.V.Rao MD
PNEUMOCOCCAL PNEUMONIA MORTALITY 8%-10% Overall healthy young adults (non bacteriemic) < 1% Bacteriemic pneumonia: 15%-20% High-risk groups:50% Elderly > 70 years: 30%-40% Young adults (<45 years): <8% Dr.T.V.Rao MD
Treatment • Penicillin (penicillin G/amoxicillin) remains the drug of choice for strains that are fully sensitive • Cefotaxime and ceftriaxone are the first-line alternatives in cases with higher levels of resistance. Dr.T.V.Rao MD
Treatment • Treatment is usually with Beta-lactam antibiotics. In the 1960s, nearly all strains of S. pneumoniae were susceptible to penicillin, but since that time, there has been an increasing prevalence of resistance, especially in areas of high antibiotic use. A varying proportion of penicillin-resistant strains may also be resistant to erythromycin, macrolides, and clindamycin and the quinolones. Dr.T.V.Rao MD
ORAL ANTIBIOTICS • Amoxicillin: first choice in < 5 years • Alternatives: co-amoxiclav, azithromycin, cefaclor, erythromycin, clarithromycin • > 5 years. • Macrolide antibiotics should be used if either mycoplasma or chlamydia pneumonia is suspected • Amoxicillin should be used as first line treatment at any age if S pneumoniae is thought to be the likely pathogen. Dr.T.V.Rao MD
IV antibiotics • Indications of Intravenous antibiotics • Unable to take oral antibiotics (for example, because of vomiting) • presents with severe signs and symptoms. • Antibiotics: • co-amoxiclav, cefuroxime, and cefotaxime. Dr.T.V.Rao MD
Vancomycin is helpful in resistant strains • Most remain susceptible to vancomycin, which is a less desirable antibiotic because of dosing and tissue penetration issues. Susceptibility testing is routine, with empiric antibiotic treatment, guided by resistance patterns in the community in which the organism was acquired, pending the results. Dr.T.V.Rao MD
PNEUMOCOCCAL POLYSACCHARIDE VACCINEs • 14-valent pneumococcal vaccine licensed in 1977 • 23-valent preparation licensed in 1983 • 23-valent vaccines cover 85%-90% of serotypes that cause invasive pneumococcal infections • 23-valent vaccines contain serotypes 1, 2, 3, 4, 5, 6B, 7F, 8, 9N, 9V, 10A, 11A, 12F, 14, 15B, 17F, 18C, 19A, 19F, 20, 22F, 23F, and 33F • 6 serotypes most frequently associated with drug-resistant infection: 6B, 9V, 14, 19A, and 23F Dr.T.V.Rao MD
23-valent Pneumococcal Polysaccharide VaccinePPV23 • 25 µg of purified capsular polysaccharide antigen serotypes: 1, 2, 3, 4, 5, 6B, 7F, 8, 9N, 10A, 11A, 12F, 14, 15B, 17F, 18C, 19A, 19F, 20, 22F, 23F, 33F • Covers 85-90% of invasive pneumococcal disease • Relatively good antibody responses (60–70%) following a single intramuscular/subcutaneous immunization in most healthy adults Dr.T.V.Rao MD
PPV23Recommendations • For healthy adults 65 years of age, particularly those living in institutions - Based on data from observational studies: significant protective effect against IPD, but not pneumonia - Based on data from randomised controlled trials: failed to show a beneficial effect of the vaccine • Persons 2 years at higher risk of PID (asplenic, immunocompromised, …) Dr.T.V.Rao MD
7-valent Pneumococcal Conjugated Vaccine PCV7 • Seven S. pneumoniae capsular polysaccharide antigens, • conjugated to nontoxic diphtheria toxin • (cross-reactive material, CRM(197) • CRM(197): inert but immunogenic variant of diphtheria toxoid • also used as a carrier molecule in one H.influenzae type b • conjugate vaccine Dr.T.V.Rao MD
PCV7. Characteristics • higher antibody levels and a more efficient immune response in infants • significant immunological memory • >90% effective against invasive disease • less effective against other forms of the disease (non-invasive pneumonia, otitis media, …) Dr.T.V.Rao MD
PCV7.Safety and schedule • 2, 4, 6 months, booster 12-14 months • Possible interference with other conjugate vaccines (meningococcal) when administered together • Safe • Adverse reactions: fever Dr.T.V.Rao MD
CDC RECOMMENDATIONS • Immunocompromised persons >2 years with: Functional or anatomic asplenia HIV, AIDS Leukemia, lymphoma, Hodgkin’s disease, multiple myeloma Generalized malignancy Chronic renal failure, nephrotic syndrome Receiving immunosuppressive chemotherapy, radiation Organ and bone marrow transplant patients Dr.T.V.Rao MD