Download
1 / 41
440 likes | 605 Views
To Perform Optimal Spirometric Measurement. Ass.Prof.Dr.Gaye Ulubay Baskent University School of Medicine Dept. of Pulmonary Diseases. Overview. Definition History of spirometry Why needed standardisation? Equipment Acceptability Repeatability Test selection. Description.

E N D
To Perform Optimal Spirometric Measurement Ass.Prof.Dr.Gaye Ulubay Baskent University School of Medicine Dept. of Pulmonary Diseases
Overview • Definition • History of spirometry • Why needed standardisation? • Equipment • Acceptability • Repeatability • Test selection
Description • Pulmonary function testings (PFTs) are maneuvers to measure airflow and lung volumes using standardized equipments
History of Spirometry • 1846 Hutchinson water spirometer • 1933 Hermannsen MVV • 1948 Normal predicted values of MVV determined • 1947 Tiffeneau and Pinelli FVC • 1955 Leuallen and Fowler FEF 25-75%
1979 Standardization of PFTs by ATS • 1987 Spirometry standards revised • 1991Reference values & interpretation • 1993 ERS standards • 1994 BTS standards • 1994 ATS standards revised • 2005ATS/ERS Task Force:General Laboratory, spirometry,diffusion capacity, lung volumes and interpretation
Why do we need to standards? • to reduce the noise on the signal • to ensure data are universally comparable • The standards • should not limited obtaining data on an individual • should not over ride common sense
Standardization • Availability of equipment • Calibration control • Measurement • Acceptability • Repeatability • Reference values • Interpretation
Contraindications • Patients should not be tested within 1 month of a myocardial infarction
Conditions which test could be suboptimal • Abdominal or chest pain of any causes • Oral or facial pain exacerbated by a mouthpiece • Stress incontinence • Dementia or confusial state
Laboratory • Ambient temperature, pressure and time of day must be recorded • Test should not performbelow 17 Cº • Same equipment for repeat testing • Same technician, same time of day • Technicians should be trained once for each 3-5 years
Equipments • The spirometer must be capable of measuring volume for 15s • Measuring volumes of 8L with an accuracy of at least 3 % or 0.050 L • Total resistance to airflow at 14L/s must be <1.5cmH2O/L/s
Syringe should be stored and used in a same ambient conditions with the spirometer • Syringe should be checked for leak monthly
Ambient temperature should be 17-40 oC during calibration and tests • Air leaks should be checked every day • Leaks should be checked by applying a constant pressure of 3cmH2O
Predicted values • Weight • Age (year) • Height • Gender • Subjects with a deformity of thoracic cage Height = arm span distance/1.06
Should not smoke within at least 1h of testing Should not consume alcohol within 4 h of testing Should not performe vigorous exercise within 30 min of testing Should not wear strict clothes Should not eat a large meal within 2 hours of testing Bronchodilator medications? Before test
During test • Sitting or standing position • Upright sitting • Nose clip • Army chair • Wheelchair? • Obesity? • False teeth?
During test • Should be rest 5-10 min. • Should be relaxed • Should be informed on tests
Recommended order of tests • Dynamic studies: spirometry, flow volume loop, PEF • Static lung volumes • Diffusing capacity • Bronchodilator test
In spirometry; • First step is maximum inspiration • Second step is maksimum forced expiration
Acceptability criteriasATS/ERS Task Force 2005 No artefacts on spirogram: • Should not cough • Should not close glottis within 1s of exhalation • Should not terminate test early • Should not perform variable effort • Should not leak from mouthpiece • Should not close of openness by mouthpiece
BACK EXTRAPOLATION 4 ZERO TIME (EV) MAXIMAL INSPIRATORY LEVEL 3 EXTRAPOLATED VOLUME 2 VOLUME, L 1 0 1 2 3 4 TIME, s Start of test must be rapid Extrapolation volume • Ekstrapolation volume must be < 5% of FVC or 0.150 L • A pause of < 1s at TLC after inspirium
End of test criteria Exhalation: • Exhalation time must be 6s and/or a plateau must be seen in volume time curve • The patient cannot continue further exhalation • No change in volume for 1 s at the end of exhalation • Time could be prolonged in patients with obstruction or older subjects
Quality control of test • Volume –time display • Flow- volume display
Acceptable Spirogram Volume-Time Flow-Volume
Cough in 1second Volume-Time Flow-Volume
Glottic closure Volume-Time Flow-Volume
Variable effort Early termination Volume-Time Flow-Volume
Air leak Volume-Time Flow-Volume
Spirometry Acceptability CriteriasATS/ERS Task Force 2005 Three acceptable spirograms • The largest values of FVC must be < 0.150 L of each other • The largest values of FEV1 must be < 0.150 L • For those with an FVC of ≤ 1 L both these values are 0.100L If both of these criteria do not meet Continue testing until • Both criteria are met with acceptable spirograms • A total 8 tests have been performed • The patient cannot continue
Test selection • Three tests with acceptable start of test and free from artefact are selected and saved • The largest FVC and the largest FEV1 should be recorded and FEV1 /FVC should be calculated
Test appropriate for the repeatability criterias Volume-Time Flow-Volume
Test not appropriate for the repeatability criterias Tekrarlanabilirlik Kriterine Uygun Olmayan Test TEKRARLANABİLİRLİK Volume-Time Flow-Volume
FVC Maneuver No Met within acceptability criteria? Yes No 3 acceptability manoeuvers? Yes No Met between repeatibilty criteria? Yes Determine the largest FVC and largest FEV1 Select maneouvre with largest FVC+ FEV1 Interpret Standardisation
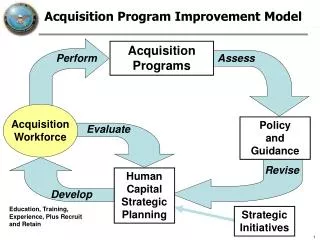
Equipment performance criteria Equipment validation Quality control Perform maneuver Measurement procedures Acceptability Repeatability Reference value/ interpretation Clinical assessment Feedback to technician Quality assessment